Three passengers are dead. A man lies in intensive care in South Africa, fighting for his life. And a Dutch expedition cruise ship, carrying 147 people of 23 nationalities, is adrift in the Atlantic Ocean, denied entry to multiple ports, transformed overnight from a vessel of adventure into a floating quarantine zone.
This is not a plot from a disaster thriller. This is the MV Hondius, May 2026, and the world is watching.
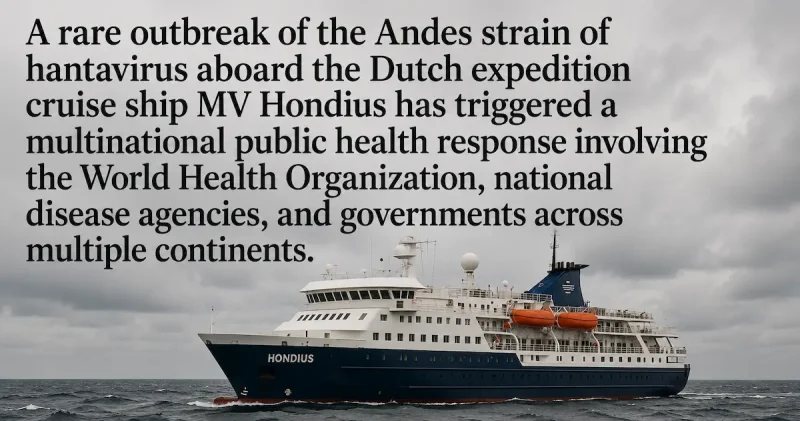
A rare outbreak of the Andes strain of hantavirus, the only known hantavirus capable of human-to-human transmission, has erupted aboard the Dutch-flagged expedition cruise ship MV Hondius, operated by Oceanwide Expeditions, igniting a multinational public health emergency that has drawn in the World Health Organization, national disease agencies, and governments spanning Europe, Africa, and Latin America. What began as a birdwatching voyage through some of the most remote and ecologically spectacular corners of the South Atlantic has become one of the most closely scrutinized infectious disease events of 2026.
The vessel departed Ushuaia, Argentina, on 1 April 2026, carrying 88 passengers and 59 crew members on an ambitious itinerary that wound through mainland Antarctica, South Georgia, Nightingale Island, Tristan da Cunha, Saint Helena, and Ascension Island. By the time alarm bells rang in Geneva, the first patient had already been dead for weeks, his body removed from the ship at Saint Helena, and his wife had collapsed on a flight to Johannesburg, dying upon arrival. Laboratory testing in South Africa would confirm what investigators feared: hantavirus infection, a hemorrhagic zoonotic virus with a case fatality rate reaching up to 50 percent in the Americas.
As WHO Director-General Dr. Tedros Adhanom Ghebreyesus briefed journalists in Geneva on 7 May 2026, the toll stood at eight cases, five laboratory-confirmed, three suspected, with three dead, one critically ill, and an entire planet bracing for answers to a single urgent question: how did one of the rarest and most feared viruses in the Americas end up spreading among passengers on a luxury expedition cruise ship in the middle of the Atlantic Ocean?
The outbreak has exposed the razor-thin margin between an isolated tragedy and a genuine global health crisis. It has tested the International Health Regulations, the binding global framework designed for exactly these moments. It has forced sovereign nations to make agonizing decisions about solidarity versus self-preservation. And it has flooded social media with the kind of pandemic-era panic that public health officials have been dreading since COVID-19 reshaped the world's threat perception forever.
Yet the scientists are urging calm. According to Nature, infectious disease researchers stress that hantaviruses carry no pandemic potential, that transmission requires close, prolonged contact, and that existing containment tools, contact tracing, isolation, monitoring, are well-understood and effective. WHO's acting director for epidemic and pandemic management, Maria Van Kerkhove, was unambiguous: "This is not SARS-CoV-2. This is not the start of a COVID pandemic."
But the dead are real. The fear is real. And the questions, about how this virus reached a ship, who else may have been exposed across five continents, and whether the world's public health infrastructure can handle a fast-moving, multi-country outbreak aboard a vessel carrying two dozen nationalities, demand answers that only a full investigation will provide.
What follows is a comprehensive account of everything we know: the virus, the ship, the victims, the science, and the extraordinary international response that has put the MV Hondius at the center of the world's most urgent public health story.
What Happened on the MV Hondius: Timeline of the Outbreak, Passenger Exposure, and Shipboard Response
To understand how a deadly hemorrhagic virus came to stalk the corridors of a Dutch expedition cruise ship in the middle of the Atlantic Ocean, you have to start not at sea, but in the wilderness of southern South America, weeks before the MV Hondius ever left port.
Before the Ship: Argentina, Chile, and Uruguay
The passengers who would become the outbreak's first known victims had not simply flown into Ushuaia and boarded. According to WHO's Disease Outbreak Notice, the couple, identified in public health documents only as Case 1 and Case 2, had traveled extensively through Argentina, Chile, and Uruguay prior to embarkation on 1 April 2026. Their itinerary included visits to sites where the rodent species known to carry the Andes strain of hantavirus is present. They were birdwatchers, drawn to the extraordinary avian richness of Patagonia and the South Atlantic, exactly the kind of rural, ecologically immersive travel that brings people into proximity with the small mammals whose urine, droppings, and saliva harbor one of the hemisphere's most lethal viruses.
This pre-boarding exposure window is critical. As Nature reported, Rhys Parry, a molecular virologist at the University of Queensland, noted that symptoms typically appear between one week and one month after exposure, meaning passengers could have contracted the disease before they boarded, during offshore excursions at remote stops along the route, or conceivably aboard the ship itself. The Andes hantavirus incubation period can stretch to six, or in some documented cases, eight weeks, a biological time delay that would prove profoundly consequential for the outbreak's detection and containment.
Crucially, Argentina had been experiencing an ongoing Andes virus outbreak since at least mid-2025. Between July 2025 and January 2026, at least 20 deaths from the virus were reported in the country, with the case fatality rate rising sharply, reaching 34% between January 2025 and January 2026, compared to historical national averages of 10–32% in each year from 2019 to 2024, according to Argentina's Ministry of Health. The ship departed from Ushuaia, in the far south of the country, more than 1,500 kilometers from the regions where active circulation was being tracked, but investigators could not rule out that the virus had spread further south than official surveillance had detected, or that the index cases had been exposed further north during their overland travel.
1 April 2026: Departure from Ushuaia
The MV Hondius, operated by the Dutch company Oceanwide Expeditions, sailed from Ushuaia, Argentina, on 1 April 2026, carrying a total of 147 individuals: 88 passengers and 59 crew members representing 23 nationalities. Its planned itinerary was the kind that draws serious expedition travelers, not sunbathers and casino-goers, but naturalists, wildlife photographers, and polar enthusiasts willing to pay a premium for access to some of the most remote ecosystems on Earth.
The route wound through mainland Antarctica, South Georgia, Nightingale Island, Tristan da Cunha, Saint Helena, and Ascension Island, before heading north toward Cabo Verde. These are not ordinary tourist destinations. They are among the most ecologically sensitive, biologically rich, and logistically challenging locations on the planet, places where passengers routinely disembark in small boats, wade ashore on wildlife beaches, and explore terrain far beyond the reach of conventional tourism infrastructure. The extent to which passengers came into contact with local wildlife or rodent habitats during these shore excursions remains, as of the time of this reporting, undetermined by investigators.
6 April 2026: First Symptoms Appear
Five days into the voyage, the man who would become Case 1 fell ill. According to WHO's outbreak documentation, he developed symptoms of fever, headache, and mild diarrhea on 6 April 2026 while aboard the ship. These are the classic prodromal signs of hantavirus cardiopulmonary syndrome, nonspecific, easily confused with influenza or a gastrointestinal bug, and offering no obvious signal that something catastrophic was underway.
At this stage, there was no reason for the ship's medical team to suspect hantavirus. The virus is rare, the symptoms are generic, and the clinical picture had not yet evolved into the terrifying respiratory collapse that characterizes advanced hantavirus cardiopulmonary syndrome. The ship continued its voyage.
11 April 2026: First Death Aboard the Vessel
By 11 April, Case 1's condition had deteriorated with brutal speed. He developed acute respiratory distress, the hallmark of hantavirus cardiopulmonary syndrome in its late, life-threatening phase, and died aboard the vessel on the same day. No microbiological tests were performed at the time of death. Without laboratory confirmation, the cause of death remained uncertain. The body was removed from the vessel at Saint Helena, a British Overseas Territory, on 24 April.
This gap, between the first death and any diagnostic confirmation, would have enormous consequences. It meant that for nearly three weeks after Case 1 died, the ship continued moving, passengers continued mingling, and the possibility of an infectious disease outbreak aboard was not yet formally recognized. Whether enhanced onboard surveillance at this point could have detected additional cases earlier remains one of the central questions for post-outbreak review.
24 April 2026: Second Case Goes Ashore at Saint Helena
Case 2, the wife of Case 1 and his close contact throughout the voyage, went ashore at Saint Helena on 24 April 2026 with gastrointestinal symptoms. She was already deteriorating. Her condition worsened significantly during a flight to Johannesburg, South Africa, on 25 April. She died upon arrival at the emergency department on 26 April. Laboratory testing subsequently confirmed hantavirus infection by PCR on 4 May, a devastating posthumous diagnosis that retroactively reframed everything that had happened on the ship.
Contact tracing for passengers on her flight to Johannesburg was immediately initiated. A flight attendant who had come into close contact with the critically ill woman was tested, and, in a finding that offered significant reassurance about the virus's limited transmissibility, tested negative for hantavirus, according to WHO.
24–27 April 2026: Third Case Emerges, Medical Evacuation Ordered
The outbreak was not confined to the first couple. On 24 April 2026, Case 3, an adult male passenger, presented to the ship's doctor with febrile illness, shortness of breath, and signs of pneumonia. His condition worsened two days later. He was medically evacuated from Ascension Island to South Africa on 27 April, where he was admitted to an intensive care unit. An extensive respiratory pathogen panel came back negative, ruling out the most common culprits, before PCR testing confirmed hantavirus infection on 2 May 2026. As of the time of WHO's reporting, his condition was described as improving.
28 April 2026: Fourth Case Develops Symptoms
Case 4, an adult female, began experiencing fever and a general feeling of being unwell on 28 April 2026. Her condition deteriorated rapidly. She died on 2 May 2026, the third fatality connected to the outbreak, and the event that triggered the formal notification to WHO that would set the international emergency response in motion.
2 May 2026: WHO Notified, The World Learns of the Outbreak
On 2 May 2026, WHO received formal notification from the National International Health Regulations Focal Point of the United Kingdom, the first country to trigger the IHR alert mechanism, regarding the cluster of severe acute respiratory illness aboard the MV Hondius, including two deaths and one critically ill passenger. Laboratory testing in South Africa confirmed hantavirus infection in the critically ill patient on the same day. The vessel was, at this point, moored off the coast of Cabo Verde.
The picture that emerged was alarming: at least seven people had fallen ill since early April, three were dead, one was in intensive care on another continent, and three more suspected cases remained aboard a ship carrying 147 people of 23 nationalities in the middle of the Atlantic Ocean.
Onboard Response: Containment Measures Aboard the Hondius
Once the outbreak was formally recognized, the response aboard the MV Hondius shifted into emergency mode. Passengers were advised to practice maximal physical distancing and remain in their cabins where possible. Disinfection procedures were initiated throughout the vessel. Anyone developing symptoms was to be isolated immediately, with respiratory etiquette enforced and medical masks required for those with respiratory symptoms.
WHO deployed an expert aboard the ship in Cabo Verde, alongside Dutch physicians and a European disease specialist, to conduct comprehensive medical assessments of all passengers and crew and to gather critical information for evaluating infection risk. WHO also arranged for the shipment of 2,500 diagnostic kits from Argentina to laboratories in five countries to strengthen testing capacity across the multinational response network.
WHO Representative in Cabo Verde Ann Lindstrand, speaking to UN News, confirmed that medical supplies had been brought aboard to ensure that any passenger who fell ill during the transit to the Canary Islands could receive immediate care. "During the trip to the Canary Islands we have been able to bring medical supplies, so if somebody gets sick on the boat, there will be medical doctors and supplies to be able to take care of them during the journey," she said.
By the time WHO briefed the world on 7 May, the situation aboard the ship had stabilized, at least temporarily. No passengers or crew currently remaining aboard were showing active symptoms. But the incubation window had not closed. With the Andes hantavirus capable of a six-to-eight week incubation period, investigators warned that additional cases could still emerge among the hundreds of passengers who had already disembarked at stops along the route.
The Full Timeline at a Glance
| Date | Event | Location | Significance |
|---|---|---|---|
| Before 1 Apr 2026 | Index cases travel through Argentina, Chile, Uruguay; visit rodent-endemic birdwatching sites | South America | Most probable window of initial viral exposure |
| 1 April 2026 | MV Hondius departs Ushuaia with 147 passengers and crew of 23 nationalities | Ushuaia, Argentina | Voyage begins; exposed individuals already aboard |
| 6 April 2026 | Case 1 (adult male) develops fever, headache, mild diarrhea | Aboard MV Hondius | First recorded symptom onset; no hantavirus diagnosis at this stage |
| 11 April 2026 | Case 1 develops acute respiratory distress and dies aboard the vessel; no microbiological testing performed | Aboard MV Hondius | First death; cause of death unconfirmed; ship continues voyage |
| 24 April 2026 | Case 1's body removed at Saint Helena; Case 2 (his wife) goes ashore with gastrointestinal symptoms; Case 3 presents to ship's doctor with fever and pneumonia signs | Saint Helena (British Overseas Territory) | Multiple cases now apparent; medical response escalates |
| 25–26 April 2026 | Case 2 deteriorates on flight to Johannesburg; dies on arrival at emergency department in South Africa | South Africa | Second death; flight contact tracing initiated |
| 27 April 2026 | Case 3 medically evacuated from Ascension Island to South Africa; admitted to ICU | Ascension Island / South Africa | First surviving patient requiring intensive care; critical test case for containment |
| 28 April 2026 | Case 4 (adult female) develops fever and malaise | Aboard MV Hondius | Fourth case emerges; outbreak accelerating |
| 2 May 2026 | Case 4 dies; PCR confirms hantavirus in Cases 2 and 3; UK notifies WHO under IHR; three suspected cases remain aboard; vessel moored off Cabo Verde | Cabo Verde / South Africa | Formal outbreak declaration; international response triggered |
| 4 May 2026 | WHO publishes Disease Outbreak Notice; seven cases reported (2 confirmed, 5 suspected); Institut Pasteur de Dakar engaged for additional testing | Geneva / Dakar | WHO activates three-level coordination; global public health machinery engaged |
| 7 May 2026 | WHO Director-General briefs media; eight cases confirmed or suspected; WHO expert boards ship; 2,500 diagnostic kits shipped to five countries | Geneva / Cabo Verde | Full international response publicly disclosed; WHO stresses low pandemic risk |
| 8 May 2026 | Flight attendant who handled Case 2 tests negative; WHO reaffirms "absolutely low" wider outbreak risk; vessel en route to Tenerife, Canary Islands | Atlantic Ocean / Geneva | Key negative test result bolsters limited transmissibility assessment; disembarkation planning underway |
The Unanswered Question: Where Did the Virus Board the Ship?
The central epidemiological mystery, the question that will define the outcome of the investigation, is precisely when and where the index cases were infected. The leading hypothesis, supported by the known travel history of Cases 1 and 2, is that they inhaled aerosolized rodent excreta during their pre-boarding birdwatching trip through hantavirus-endemic areas of South America. As molecular virologist Rhys Parry of the University of Queensland told Nature, any outbreak on the ship most likely resulted from contact with material from an infected rodent, rather than from person-to-person transmission, with several people potentially exposed through the same contaminated area.
But a secondary possibility has not been ruled out. The MV Hondius made stops at remote, ecologically rich islands, Nightingale Island and Tristan da Cunha among them, where passengers went ashore and engaged with wild environments. WHO's outbreak notice specifically noted that the extent of passenger contact with local wildlife during the voyage, or prior to boarding in Ushuaia, remains undetermined. The possibility that rodent reservoirs at one or more of the ship's remote port calls provided an additional, or even the primary, source of exposure cannot be excluded until environmental sampling and sequencing data are complete.
What is clear is that by the time the world knew the ship had a problem, the virus had already claimed three lives, crossed international borders on commercial aircraft, and seeded cases across multiple continents. The MV Hondius had become something its designers never imagined: a mobile index event in a global outbreak investigation.
Understanding Andes Strain Hantavirus: Symptoms, Transmission Risks, Mortality Rate, and How It Differs from Other Hantaviruses
To grasp why the outbreak aboard the MV Hondius has triggered such an intense international response, and equally, why scientists are insisting it does not portend a pandemic, you need to understand the precise nature of the pathogen at its center. The Andes strain of hantavirus is not just another respiratory virus. It is, in the taxonomy of known human pathogens, something genuinely unusual: a rodent-borne hemorrhagic virus with a lethality rate that can reach 50 percent in the Americas, a clinical trajectory that moves from vague flu-like symptoms to catastrophic lung failure within days, and, uniquely among all known hantaviruses, a documented, if limited, capacity to jump from person to person.
That last characteristic is what makes this outbreak different from most hantavirus incidents. And it is what makes the MV Hondius case worth understanding in detail.
The Hantavirus Family: Old World and New World
Hantaviruses are a large and diverse family of zoonotic viruses, pathogens that circulate primarily in animal reservoirs but can infect humans under the right conditions. According to Nature, they divide broadly into two groups defined by geography and the distinct disease syndromes they cause in humans.
The Old World hantaviruses, found across Africa, Asia, and Europe, primarily cause hemorrhagic fever with renal syndrome (HFRS), a disease characterized by fever, bleeding abnormalities, kidney failure, and shock. In East Asia, particularly China and the Republic of Korea, HFRS continues to account for thousands of cases annually, though incidence has declined in recent decades. In Europe, 1,885 hantavirus infections were reported in 2023, marking the lowest rate observed between 2019 and 2023, according to WHO. Old World strains do not spread between people.
The New World hantaviruses, found in the Americas, cause a fundamentally different and frequently more lethal syndrome: hantavirus cardiopulmonary syndrome (HCPS), also known as hantavirus pulmonary syndrome (HPS). In North America, Sin Nombre virus is the predominant cause. In South America, and specifically in Argentina and Chile, the dominant strain is Orthohantavirus andesense, better known as the Andes virus. It was first identified in 1995, and it carries a clinical profile that places it among the most dangerous respiratory pathogens in the Western Hemisphere.
| Characteristic | Old World Hantaviruses (e.g., Puumala, Hantaan) | New World Hantaviruses (e.g., Sin Nombre) | Andes Virus (New World) |
|---|---|---|---|
| Primary geographic distribution | Europe, Asia, Africa | North America | South America (Argentina, Chile) |
| Disease caused in humans | Hemorrhagic fever with renal syndrome (HFRS) | Hantavirus cardiopulmonary syndrome (HCPS/HPS) | Hantavirus cardiopulmonary syndrome (HCPS/HPS) |
| Primary organ system affected | Kidneys, vascular system | Lungs, cardiovascular system | Lungs, cardiovascular system |
| Case fatality rate | <1–15% | Up to 38% | Up to 50% in some outbreak settings |
| Human-to-human transmission documented | No | No | Yes, limited, documented in community settings |
| Approved vaccine available | No (for most strains) | No | No |
| Approved antiviral treatment | Ribavirin (for HFRS, limited evidence) | None approved | None approved |
| Rodent reservoir | Various (bank vole, striped field mouse) | Deer mouse (Peromyscus maniculatus) | Long-tailed pygmy rice rat (Oligoryzomys longicaudatus) |
How the Andes Virus Infects: The Route from Rodent to Human
In the overwhelming majority of cases, humans contract hantavirus not from other people but from rodents, specifically through exposure to the urine, feces, or saliva of infected animals. According to the WHO Disease Outbreak Notice, transmission typically occurs when aerosolized particles of contaminated rodent excreta are inhaled, a mechanism that makes enclosed, poorly ventilated spaces particularly dangerous. Touching contaminated surfaces and then touching the mouth, nose, or eyes can also transmit the virus, though inhalation is the primary route.
High-risk activities include cleaning buildings or outbuildings with rodent infestations, camping or hiking in areas where infected rodents are present, and agricultural or forestry work in endemic regions. As Nature reported, any outbreak on the MV Hondius most probably resulted from initial contact with infected rodent material, not from person-to-person spread, with multiple individuals potentially exposed through the same contaminated environment during their South American travels.
The Andes virus reservoir in South America is the Oligoryzomys longicaudatus, the long-tailed pygmy rice rat, a small rodent whose range spans Chile and Argentina and whose population dynamics are closely tied to environmental and climatic conditions. Periods of high rainfall and food abundance can drive rodent population surges, increasing human exposure risk, a pattern that likely contributed to the elevated case fatality rates observed in Argentina between 2025 and 2026.
The Clinical Progression of Andes Hantavirus Infection: From Prodrome to Crisis
What makes hantavirus cardiopulmonary syndrome so clinically treacherous is the gap between its benign early presentation and the catastrophic speed of its late-stage deterioration. Physicians who are not specifically alert to the possibility of hantavirus infection can easily misread the initial symptoms as influenza, gastroenteritis, or a generic respiratory illness, and by the time the true diagnosis becomes apparent, the patient may already be in irreversible respiratory collapse.
WHO's clinical description of HCPS outlines a characteristic two-phase course that clinicians must recognize:
The prodromal phase, lasting typically three to five days, is characterized by fever, headache, dizziness, chills, myalgia (severe muscle pain), and gastrointestinal symptoms including nausea, vomiting, diarrhea, and abdominal pain. There are no respiratory symptoms at this stage. A patient presenting with these symptoms in an emergency department, absent a specific travel history and clinical suspicion, would rarely prompt immediate hantavirus testing. This is precisely the clinical picture that Case 1 aboard the MV Hondius presented before his death: fever, headache, mild diarrhea, the textbook prodrome of a virus that was about to kill him.
The cardiopulmonary phase arrives with devastating suddenness, typically within hours of the end of the prodromal period. The hallmark is the abrupt onset of respiratory distress driven by acute pulmonary edema: the lungs fill with fluid as vascular permeability collapses across the entire capillary bed. Hypotension and shock follow rapidly. Without immediate intensive care support, mechanical ventilation, aggressive hemodynamic monitoring, vasopressors, and in the most severe cases extracorporeal membrane oxygenation (ECMO), death can occur within hours of respiratory decompensation.
The incubation period before any symptoms appear ranges from one week to eight weeks following exposure, with most cases presenting within two to four weeks. WHO specifically warned that the MV Hondius outbreak's incubation window meant additional cases could still emerge among the hundreds of passengers who had already disembarked at ports along the route, a biological clock that could not be stopped once the exposure had occurred.
The Mortality Rate: Up to 50 Percent in the Americas
The case fatality rate for hantavirus infection varies dramatically by strain and geography. In Europe and Asia, it runs below 1 to 15 percent. In the Americas, it reaches up to 50 percent, a figure that places HCPS among the most lethal acute respiratory syndromes known to medicine. WHO's 2025 data from the Americas recorded 229 cases and 59 deaths across eight countries, a case fatality rate of 25.7 percent. In Argentina specifically, the situation had worsened: between January 2025 and January 2026, 34 percent of infected individuals died, significantly above the historical national average.
What drives this lethality is the absence of any approved specific antiviral treatment. Ribavirin has demonstrated efficacy against HFRS, the Old World syndrome, but has not shown effectiveness against HCPS and is not licensed for either treatment or prophylaxis of hantavirus pulmonary syndrome. There is no approved vaccine for any hantavirus strain. Treatment is entirely supportive: careful fluid administration, hemodynamic monitoring, respiratory support, mechanical ventilation, and in severe cases, ECMO. Survival depends almost entirely on how quickly a patient reaches a facility capable of providing that level of care, and how aggressively and expertly the clinical team manages the rapid cardiopulmonary deterioration.
In the context of the MV Hondius outbreak, this reality has profound implications. The first patient died at sea, without any confirmed diagnosis and without access to ICU-level care. The second patient deteriorated and died in transit to hospital. The third patient, medically evacuated to South Africa, survived in intensive care, his condition improving. The difference between survival and death, in Andes hantavirus infections, often reduces to hours and geography.
The Defining Characteristic: Human-to-Human Transmission
Among everything that distinguishes the Andes virus from the rest of the hantavirus family, one characteristic stands apart as both scientifically remarkable and epidemiologically consequential: it is the only known hantavirus capable of limited human-to-human transmission.
WHO is explicit on this point: the Andes strain can spread between people, but transmission generally requires close and prolonged contact, the kind typical of household members, intimate partners, or healthcare workers providing direct care to an infected patient without adequate personal protective equipment. This is not airborne transmission in the manner of influenza or SARS-CoV-2. It is not spread by casual contact, shared air in public spaces, or brief proximity to an infected individual.
The evidence for human-to-human transmission of Andes virus comes from several documented outbreak investigations, most notably a 2018–2019 outbreak in Argentina where transmission was linked to a social gathering involving a symptomatic individual, a so-called "super-spreader" event that produced only a small number of secondary cases. A landmark 2020 study in the New England Journal of Medicine by Martínez and colleagues documented the dynamics of such events in detail, establishing the epidemiological parameters that now guide outbreak response.
The critical qualifier is what "limited" transmission actually means in practice. WHO spokesperson Christian Lindmeier was emphatic at the 8 May briefing: "Even those who have been sharing cabins don't seem to be both infected in some cases…it's not spreading anything close to how COVID was spreading." The wife of a confirmed case being treated in a Swiss hospital had self-isolated but presented no symptoms, a finding that, as Lindmeier noted, underscored the virus's comparatively low person-to-person transmissibility even in intimate household settings. A flight attendant who had handled Case 2, the critically ill woman who later died, tested negative for hantavirus, further evidence that even brief close contact with a severely symptomatic patient does not reliably transmit the virus.
WHO's acting director for epidemic and pandemic management, Maria Van Kerkhove, drew the sharpest possible distinction from COVID-19: "Hantaviruses have been around for quite a while. We know this virus. It does not spread the same way that coronaviruses do."
Why There Is No Vaccine, and What That Means
One aspect of the Andes virus outbreak that has drawn particular attention from the scientific community is the complete absence of any licensed vaccine or specific antiviral therapy. As Nature reported, Vaithi Arumugaswami, an infectious-disease researcher at the University of California, Los Angeles, called the MV Hondius incident "a warning that the viruses should be monitored and that more research is needed to develop vaccines and treatments for them." Despite hantaviruses being known to science for decades, their relative rarity, and their geographic concentration in low- and middle-income regions of South America, has historically failed to attract the sustained investment required to bring a vaccine through clinical trials to regulatory approval.
This is the paradox at the heart of hantavirus preparedness: a virus capable of killing half of those it infects, with no approved treatment and no vaccine, circulating in an era of rapid global travel and expanding ecotourism into previously remote habitats. The MV Hondius passengers who traveled to birdwatching sites in Patagonia and then boarded a ship bound for the Atlantic are not outliers. They are the leading edge of a growing population of adventure travelers whose itineraries increasingly intersect with zoonotic disease reservoirs in ways that existing public health infrastructure was not designed to manage.
What Clinicians and Travelers Need to Know
WHO's formal advice for individuals who may have been exposed covers several critical points: passengers and crew should monitor themselves actively for symptoms for 45 days following potential exposure; anyone developing fever, headache, muscle pain, or gastrointestinal symptoms after travel through endemic areas should seek medical attention immediately and disclose their travel history; healthcare workers treating suspected cases should apply standard and transmission-based precautions, with airborne precautions added for any aerosol-generating procedures.
Diagnosis relies on serologic testing for IgM antibodies or rising IgG titres using enzyme-linked immunoassay (ELISA), or on reverse transcriptase PCR to detect viral RNA, the method that confirmed infections in Cases 2 and 3 aboard the Hondius. Early diagnosis is not merely informative; it is potentially life-saving, because the window between symptom onset and cardiopulmonary collapse can be measured in days, and rapid transfer to an ICU-capable facility is the single most important determinant of survival.
Preventive measures for travelers in endemic regions are straightforward but require deliberate attention: avoid contact with rodents and their nesting materials, use wet-cleaning methods rather than dry sweeping when cleaning enclosed spaces (which can aerosolize contaminated dust), ensure proper ventilation, store food in rodent-proof containers, and wear appropriate protective equipment when working in environments with known rodent activity. Most routine tourism activities, WHO notes, carry little or no risk, it is the specific combination of rural, ecologically immersive environments and close proximity to rodent habitats that elevates exposure risk to meaningful levels.
For the passengers of the MV Hondius, many of whom had already disembarked across multiple continents before the outbreak was formally declared, the clinical message was urgent: the incubation clock was still running, and anyone who had traveled through South America before boarding, or who had gone ashore at any of the ship's remote island stops, needed to know what symptoms to watch for, and how little time they might have to act if those symptoms appeared.
Why This Case Is Unusual: Person-to-Person Transmission Concerns and the Implications of a Cruise Ship Setting
In the long and grim catalog of hantavirus outbreaks recorded since the virus was first characterized in the Americas in the 1990s, the MV Hondius case stands apart. Not because of its death toll, three fatalities, though devastating, is modest by the scale of some documented Andes virus events in Argentina and Chile. Not because of the virus itself, whose biology is well understood. But because of the specific, almost improbable combination of factors that converged aboard a Dutch expedition cruise ship in the South Atlantic: a pathogen with a rare capacity for human-to-human transmission, a closed floating environment that concentrates close contact among people of two dozen nationalities, a voyage through some of the world's most remote and least-monitored ecosystems, and a passenger population already dispersed across multiple continents before a single confirmed laboratory diagnosis had been made.
Each of those factors, taken alone, would be concerning. Together, they produced something that public health systems are not well-designed to handle: an outbreak that was simultaneously low-risk in absolute epidemiological terms and extraordinarily difficult to contain logistically, legally, and diplomatically.
The Human-to-Human Transmission Question: What We Know, and What Remains Unresolved
At the center of every concern about the MV Hondius outbreak sits a single, scientifically established but epidemiologically uncomfortable fact: the Andes strain of hantavirus is the only known hantavirus capable of limited human-to-human transmission. Every other member of the hantavirus family, Sin Nombre in North America, Puumala in Scandinavia, Hantaan in East Asia, spreads exclusively from rodents to humans. The Andes virus does not follow this rule. Under conditions of close and prolonged contact, it can move between people.
That qualification, close and prolonged, carries enormous weight. It is the difference between a virus that might sustain epidemic chains under certain social conditions and one that will almost certainly extinguish itself at the household level. WHO's own data from the MV Hondius response illustrated this restraint with striking clarity: a flight attendant who handled a critically ill, visibly deteriorating infected passenger, close enough, long enough to constitute a genuine exposure event, tested negative for hantavirus. Cabin-mates of confirmed cases remained uninfected in some instances. The wife of one confirmed patient who was being treated in a Swiss hospital had not developed symptoms despite the intimate and sustained nature of household contact. These are not statistical anomalies; they reflect the fundamental transmission biology of Andes virus, which appears to require a level of contact intensity that casual proximity, even in a confined environment, does not reliably achieve.
WHO spokesperson Christian Lindmeier was direct at the 8 May briefing: "Even those who have been sharing cabins don't seem to be both infected in some cases…it's not spreading anything close to how COVID was spreading." And yet the uncertainty cannot be entirely dismissed. WHO's own Disease Outbreak Notice acknowledged that secondary infections among healthcare workers have been previously documented, that human-to-human transmission in community settings involving close and prolonged contact is an established epidemiological reality, and that the 2018–2019 Argentina outbreak demonstrated how a single symptomatic individual at a social gathering could generate a chain of secondary cases. The critical question for the MV Hondius investigation, not yet answered as of the time of this reporting, is whether any of the cases aboard the ship represent human-to-human transmission rather than independent rodent-to-human exposures from a shared contaminated environment.
This distinction matters enormously. If all cases trace back to a common rodent exposure, contaminated dust inhaled in a shared space in Argentina, or on a remote island shore, then the outbreak is, in epidemiological terms, a point-source event: terrible for those affected, but self-limiting once the exposure source is removed. If any cases represent human-to-human transmission aboard the ship, the calculus changes. Not dramatically, the transmission parameters of Andes virus make sustained chains unlikely even in a closed environment, but meaningfully enough to alter contact tracing priorities, quarantine decisions, and the duration of monitoring for the hundreds of passengers who had already left the vessel.
Molecular virologist Rhys Parry of the University of Queensland told Nature that the most probable explanation for multiple cases aboard the ship was a shared rodent exposure rather than person-to-person spread, noting that several people could have been exposed through the same contaminated area. Sequencing and metagenomics work ongoing at South African laboratories and the Institut Pasteur de Dakar were expected to shed light on whether the viral genomes from different patients share the phylogenetic signature of a single exposure event or suggest independent acquisition and possible subsequent transmission chains. Those results were not yet available at the time of publication.
The Cruise Ship as an Epidemiological Environment: Why It Amplifies Every Risk
Even setting aside the specific characteristics of the Andes virus, the cruise ship setting introduces a set of epidemiological vulnerabilities that public health officials and maritime medicine experts have long recognized, and that the MV Hondius outbreak has thrown into unusually sharp relief.
A cruise ship is, in essence, a small city with no exits. People eat together in shared dining rooms, breathe shared air in lounges and corridors, use shared bathrooms, gather on deck in close proximity, and spend days or weeks in a social environment far more intimate than any hotel or resort. For a respiratory or contact-transmitted pathogen, this is an optimal propagation environment, as the COVID-19 cruise ship outbreaks of 2020, most notoriously aboard the Diamond Princess, demonstrated with catastrophic clarity to a watching world.
The MV Hondius, however, is not a conventional cruise ship. It is an expedition vessel, smaller, more intimate, and carrying a very different passenger profile. With 88 passengers and 59 crew aboard, the social dynamics are more like those of a remote field station than a floating resort. Passengers on expedition cruises of this type tend to be highly engaged with their environment, participating together in shore excursions, wildlife observation, and communal activities that generate the kind of sustained, face-to-face social contact that, in the case of a pathogen like Andes virus, represents exactly the transmission conditions that WHO describes as necessary for human-to-human spread.
| Risk Factor | Standard Land-Based Outbreak | Conventional Cruise Ship Outbreak | Expedition Cruise Ship Outbreak (MV Hondius) |
|---|---|---|---|
| Ability to isolate cases | Moderate, patients can be hospitalized, contacts dispersed | Limited, shared ventilation, confined dining and social spaces | Severely limited, small vessel, limited medical facilities, no nearby port access |
| Access to diagnostic testing | High, laboratory networks available | Low onboard; high once evacuated | Negligible onboard; reliant on international evacuation and multi-country lab networks |
| Duration of close contact among exposed individuals | Variable, depends on household and social setting | High, days to weeks of shared environment | Very high, weeks of highly immersive social and outdoor activity together |
| Geographic dispersion of exposed contacts upon event recognition | Local to regional | Global, multinational passenger manifests | Global and complex, 23 nationalities, prior shore stops across remote territories |
| Port access for medical evacuation | Not applicable | Moderate, major ports generally accessible | Extremely limited, remote itinerary; multiple ports refused entry; nearest viable port hundreds of nautical miles away |
| Rodent exposure risk (for zoonotic pathogens) | Depends on environment | Low, passengers rarely exposed to wildlife | High, shore excursions to remote, ecologically rich islands with active wildlife contact |
| Regulatory jurisdiction for public health response | Clear national authority | Complex, flag state, port state, passenger nationalities | Extremely complex, Dutch-flagged vessel, British IHR notification, South African lab confirmation, Cabo Verde port refusal, Spanish disembarkation, 23 nationalities |
The MV Hondius's specific itinerary added layers of complexity that a conventional cruise would never face. The ship had called at mainland Antarctica, South Georgia, Nightingale Island, Tristan da Cunha, Saint Helena, and Ascension Island before the outbreak was formally declared. These are not places with hospitals, laboratories, or meaningful public health infrastructure. Tristan da Cunha, one of the most remote permanently inhabited islands on Earth, has a population of roughly 250 people and no airstrip. Nightingale Island is uninhabited. If a passenger had collapsed with acute respiratory failure at any of these stops, the medical options would have been limited to whatever the ship's own medical bay could provide, and whatever emergency evacuation could be arranged across hundreds or thousands of nautical miles of open ocean.
The case of Patient 3 illustrates how fine this margin can be. Medically evacuated from Ascension Island to South Africa, he survived, at the time of reporting, his condition was improving in an ICU. But the logistics of that evacuation, in one of the most remote corners of the Atlantic, required resources and coordination that would be impossible to replicate at every point along an expedition itinerary that deliberately seeks out the world's most inaccessible places. Patient 1 did not survive. He died aboard the ship, undiagnosed, before any evacuation could be attempted. The difference between those two outcomes may well come down to where, exactly, along the ship's track each patient's condition deteriorated beyond what the onboard medical facility could manage.
The Passenger Dispersal Problem: 23 Nationalities, Multiple Continents, and an Eight-Week Incubation Window
Among all the features of the MV Hondius outbreak that complicate the public health response, the most practically challenging may be the simplest to state: by the time the world knew there was a problem, many of the people who might have been exposed had already gone home.
The vessel carried passengers representing 23 nationalities. Some had disembarked at ports along the route, Saint Helena, Ascension Island, before the outbreak was formally declared. Others would continue to disembark as the ship made its way toward the Canary Islands. Each of these individuals had potentially been exposed to a pathogen with an incubation period of up to six to eight weeks, during which they would show no symptoms, pass through airport screening undetected, travel on commercial flights, and return to households, workplaces, and healthcare systems in countries that may or may not have been notified of their potential exposure.
Argentina's National IHR Focal Point shared passenger and crew lists with the relevant national focal points according to each person's nationality, a critical step in initiating the multi-country contact tracing effort. WHO confirmed that national health authorities were contacting passengers who had already disembarked, advising them to seek medical attention promptly if symptoms developed. WHO spokesperson Christian Lindmeier described the scope of that effort: "It's following up on everybody. It's looking into seating lists of planes, of ships, maybe even more tracing somebody's steps, seeing where they would have been or might have been in close contact."
This is contact tracing at a scale and complexity that strains even the most capable national health systems. The individuals involved are not clustered in a single community or region, they are distributed across Europe, Latin America, North America, and beyond, having arrived home through a web of international connecting flights that generate their own secondary contact networks. Each person who sat next to a symptomatic traveler on a transatlantic flight is, in principle, a contact requiring assessment, a cascade of potential exposures that multiplies with every connection in the itinerary.
The saving grace, epidemiologically, is the fundamental biology of Andes virus transmission. As WHO's data from the MV Hondius response demonstrated, even close contact with a visibly symptomatic patient, the flight attendant who handled Case 2, did not result in transmission. The requirements for human-to-human spread are stringent enough that the vast majority of contacts identified through this tracing exercise are almost certainly not at meaningful risk. But "almost certainly" is not "certainly," and in the post-COVID public health environment, the difference between those two phrases carries enormous political and social weight.
Port Refusals, Diplomatic Friction, and the Politics of Quarantine at Sea
The jurisdictional and diplomatic complications that erupted around the MV Hondius added a dimension to this outbreak that purely virological analysis cannot capture. A ship in international waters, carrying patients with a confirmed lethal infection, requesting permission to dock and disembark passengers, is not merely a medical problem. It is a political problem, a legal problem, and, in the age of social media, a reputational problem for any government that must decide whether to open its ports.
Cabo Verde declined to allow the vessel to dock, citing public health concerns, a decision that, however understandable from a domestic political standpoint, left the ship's 147 occupants in an extraordinarily difficult position: moored off the coast of an island nation, unable to land, with sick patients aboard and a floating medical crisis unfolding in real time. It fell to Spain to step forward, agreeing to allow the vessel to dock in the Canary Islands, an autonomous Spanish community, after a direct intervention by WHO Director-General Dr. Tedros, who publicly thanked Spanish Prime Minister Pedro Sánchez for what he described as an act of "solidarity" and "moral duty."
Dr. Tedros was explicit about the risk calculus: "The risk to the people of the Canary Islands is actually low." But the political symbolism of the moment was not lost on anyone watching. A country's willingness to allow a disease-stricken vessel to dock, when the science clearly supports doing so safely, is not merely a public health decision. It is a statement about how a nation weighs the interests of stranded international travelers against the domestic anxieties of its own population. In the post-COVID political environment, those anxieties are not trivial, and no government navigates them without political cost.
The IHR framework, the binding international legal architecture that governs exactly these situations, explicitly advises against travel and trade restrictions beyond those warranted by the scientific evidence. WHO's Disease Outbreak Notice stated clearly that the organization "advises against the application of any travel or trade restrictions based on the current information available on this event." Cabo Verde's refusal did not violate the letter of international law, port entry decisions involve sovereign discretion, but it created exactly the kind of diplomatic friction that IHR coordination is designed to prevent, and it underscored how much the system's effectiveness depends on political will that no treaty can fully compel.
The Disinformation Dimension: Social Media, Pandemic Trauma, and the Amplification of Fear
Complicating the public health response to the MV Hondius outbreak was a factor that would have been largely absent from outbreak management even a decade ago: the instantaneous, global amplification of fear and misinformation through social media, in a population whose pandemic threat perception has been permanently altered by COVID-19.
The parallels between the MV Hondius situation and the early days of COVID-19, a novel-seeming outbreak on an international conveyance, sick passengers being evacuated across multiple countries, governments refusing entry to affected vessels, WHO holding emergency briefings, were superficially plausible enough to generate significant online alarm. The fact that Andes virus is capable of at least limited human-to-human transmission provided a factual hook for catastrophist narratives that experts found deeply frustrating to counter.
Dr. Abdirahman Mahamud of WHO's Health Emergencies Programme addressed the disinformation directly, stressing that there were no signs of early-stage pandemic development, that the confinement of infection to a setting involving prolonged close contact was entirely consistent with known Andes virus transmission dynamics, and that existing public health tools, contact tracing, isolation, monitoring, are well understood and can effectively break transmission chains. WHO's acting director for epidemic and pandemic management Maria Van Kerkhove delivered perhaps the clearest rebuttal: "This is not SARS-CoV-2. This is not the start of a COVID pandemic. Hantaviruses have been around for quite a while. We know this virus. It does not spread the same way that coronaviruses do."
But the persistence of pandemic anxiety in the global public, entirely understandable given the trauma of 2020 and its aftermath, means that the epistemic gap between what scientists know and what the public fears does not close simply because the experts say reassuring things. Every new death, every port refusal, every image of passengers confined to their cabins becomes, in the social media ecosystem, evidence for a narrative that the official account cannot fully suppress. Managing that narrative is now an integral part of outbreak response, as demanding, in some respects, as the epidemiology itself.
What Makes This Outbreak a Warning Sign for Ecotourism and Global Travel
Stripped to its essentials, the MV Hondius outbreak is a story about the intersection of three powerful forces: the global expansion of ecotourism into previously remote and biologically rich environments; the mobility of international travelers who can carry a pathogen from a rodent burrow in Patagonia to a hospital in Johannesburg within days; and the biological reality of a virus that has been quietly circulating in South America for decades, unvaccinated against, untreatable once established, and capable, under the right social conditions, of spreading from person to person.
UCLA infectious disease researcher Vaithi Arumugaswami told Nature that while hantaviruses do not pose a pandemic risk, the MV Hondius incident is "a warning that the viruses should be monitored and that more research is needed to develop vaccines and treatments for them." The passengers aboard the Hondius were not doing anything reckless. They were doing what growing numbers of affluent, wildlife-interested international travelers do every year, visiting remote habitats to observe birds and wildlife, then boarding international transport to continue their journeys. The same itinerary, repeated by a hundred thousand travelers a year across South America's most ecologically immersive destinations, represents a standing interface between the human population and zoonotic disease reservoirs that existing surveillance systems were not built to monitor.
Argentina's ongoing Andes virus outbreak, with at least 20 deaths between July 2025 and January 2026 and a fatality rate rising above historical norms, was documented in national health ministry data. It was not a secret. Yet travelers departing from Ushuaia for a six-week Antarctic expedition cruise were not screened for hantavirus exposure risk, were not systematically advised about the symptoms to watch for, and boarded a ship whose medical facilities were not equipped to definitively diagnose or manage the disease if it emerged. The gap between what was known about the epidemiological environment and what was done with that knowledge at the point of embarkation is one the MV Hondius investigation will need to examine carefully.
The implications extend far beyond this single voyage. Expedition cruising is a growth industry. The destinations it serves, the sub-Antarctic islands, the remote Atlantic territories, the wilderness coastlines of South America, are precisely the ecosystems where zoonotic disease reservoirs are most concentrated and human public health infrastructure is most limited. As long as there is no vaccine for Andes hantavirus, no approved antiviral treatment, and no systematic pre-departure risk assessment for travelers departing from endemic regions, the conditions that produced the MV Hondius outbreak will recur. The only variable is whether the next vessel carries a more transmissible pathogen, or one that takes longer to declare itself while passengers scatter across the globe.
For now, the world has been fortunate. WHO's assessment remains that the global public health risk is "absolutely low." The dead are three. The survivors, it appears, will recover. The outbreak, by every scientific measure available, is not the beginning of a pandemic. But it is, unambiguously, a stress test, of IHR frameworks, of maritime medicine, of international diplomatic solidarity, of global contact tracing capacity, and of the public's ability to process nuanced risk communication in an environment saturated with COVID-amplified fear. On all of those fronts, the MV Hondius has exposed weaknesses that the next outbreak, whatever and whenever it turns out to be, will exploit if they are not addressed.
Multinational Public Health Response: Roles of the World Health Organization, National Disease Agencies, Contact Tracing Teams, and Governments
When the United Kingdom's National International Health Regulations Focal Point transmitted its alert to Geneva on 2 May 2026, it set in motion one of the most geographically complex, diplomatically intricate, and logistically demanding outbreak responses in recent memory. A ship in the Atlantic. Dead passengers on two continents. Confirmed hantavirus in a South African ICU. Suspected cases still aboard a vessel denied port access. And a passenger manifest representing 23 nationalities, many of whom had already scattered across the globe.
What followed was, by any measure, an extraordinary test of the international public health architecture that the world has spent decades building, and an equally extraordinary test of the political will required to make that architecture function in practice. The response engaged WHO at its highest levels, mobilized national disease agencies across multiple continents, activated contact tracing operations spanning commercial aviation networks and remote island territories, and forced sovereign governments into agonizing decisions about solidarity, sovereignty, and the limits of pandemic-era public trust.
This is the story of how the world responded, who did what, when, and with what effect.
WHO: The Architecture of a Three-Level Emergency Activation
The World Health Organization did not wait for certainty before acting. From the moment the IHR notification arrived on 2 May 2026, WHO activated what it describes as three-level coordination, a formal internal escalation that engages WHO's country offices, regional structures, and Geneva headquarters simultaneously, ensuring that the response is driven both by global strategic direction and by local operational knowledge.
The first and most visible element of WHO's response was information architecture. Within forty-eight hours of receiving the UK notification, WHO had shared outbreak information with National IHR Focal Points globally, an act of institutional transparency designed to ensure that every country in the world had the earliest possible warning that a cluster of Andes hantavirus cases was moving across international borders. On 4 May 2026, WHO published a formal Disease Outbreak Notice, placing the event on the public record and providing the detailed epidemiological situation report that national health systems needed to calibrate their own responses. By 7 May, WHO Director-General Dr. Tedros Adhanom Ghebreyesus was briefing international journalists in Geneva, flanked by WHO's most senior technical leadership.
The operational dimensions of WHO's engagement were equally significant. The organization deployed an expert directly onto the MV Hondius in Cabo Verde, a frontline epidemiologist embedded aboard the ship alongside Dutch doctors and a European disease specialist, to conduct comprehensive medical assessments of every passenger and crew member remaining aboard and to gather the clinical and epidemiological data that Geneva needed to maintain an accurate real-time risk assessment. WHO also arranged the shipment of 2,500 diagnostic kits from Argentina to laboratories across five countries, building out the testing capacity that a multi-country outbreak of this nature demands, and that no single national laboratory network, however capable, can supply unilaterally.
WHO simultaneously developed step-by-step operational guidance for the safe and respectful disembarkation and onward travel of passengers and crew upon arrival in Tenerife, a document that had to balance infection control imperatives with the legal rights and human dignity of passengers who had committed no act of negligence and whose own risk of infection was, in most cases, extremely low. This kind of operational guidance, precise, practical, respectful, and legally defensible, is unglamorous public health work. It is also exactly the kind of work that determines whether a disembarkation becomes an orderly, contained public health event or a chaotic, media-amplified disaster.
The WHO Representative in Cabo Verde, Ann Lindstrand, served as the on-the-ground operational focal point during the ship's time moored off the island nation's coast. Speaking to UN News, she described the practical dimensions of her agency's support: "During the trip to the Canary Islands we have been able to bring medical supplies, so if somebody gets sick on the boat, there will be medical doctors and supplies to be able to take care of them during the journey." Her account captures something essential about how WHO functions at its best in outbreak settings: not merely as a strategic coordinator in Geneva, but as an organization with people on the ground, in the right place, at the right time, with the right supplies.
WHO's risk communication function ran in parallel with all of this operational activity, and proved to be one of the most demanding aspects of the entire response. In a post-COVID information environment saturated with pandemic anxiety and social media amplification, the challenge of conveying a nuanced message, this virus is genuinely dangerous to those it infects; it does not pose a pandemic threat; the global public health risk is low; but we are treating this with complete seriousness, required WHO's senior leadership to perform a communication feat that has no easy template.
Maria Van Kerkhove, WHO's acting director for epidemic and pandemic management, delivered the institutional bottom line with clinical precision: "This is not SARS-CoV-2. This is not the start of a COVID pandemic. Hantaviruses have been around for quite a while. We know this virus. It does not spread the same way that coronaviruses do." Dr. Abdirahman Mahamud of WHO's Health Emergencies Programme reinforced the message directly, stressing that existing public health measures, contact tracing, isolation, and monitoring, are well understood and can effectively break chains of transmission, making a large-scale epidemic unlikely. And WHO spokesperson Christian Lindmeier deployed perhaps the most effective single piece of evidence in the entire communication arsenal: the negative test result of the flight attendant who had handled the critically ill Case 2. "Let's not forget from couples who were close…from a flight attendant who handled the sick woman who just shortly after died and was feeling extremely unwell, we get negative test results. That should convince nearly everybody now that this is a dangerous virus, but only to the person who is really infected."
The International Health Regulations: The Legal Framework That Held the Response Together
The institutional scaffolding beneath the entire multinational response was the International Health Regulations, the binding global legal framework that defines the rights and obligations of WHO member states in responding to cross-border public health events. The MV Hondius outbreak activated the IHR not as a theoretical exercise but as a live operational instrument, with multiple States Parties discharging their legal obligations in real time across multiple continents.
The United Kingdom triggered the mechanism first, notifying WHO on 2 May 2026 as the IHR Focal Point whose territory, specifically the British Overseas Territory of Saint Helena, had been the point at which Case 2 disembarked and Case 1's body was removed from the vessel. This notification was not merely procedural. It was the act that transformed a shipboard medical tragedy into an internationally recognized public health event, triggering the cascade of obligations and responses that the IHR framework is designed to produce.
Argentina's National IHR Focal Point discharged one of the most operationally critical obligations in the entire response: sharing passenger and crew lists with the National IHR Focal Points of each passenger's country of nationality. This single act, the transmission of a manifest covering 23 nationalities, was the foundation upon which every subsequent contact tracing operation across multiple countries was built. Without it, national health agencies would have been attempting to locate and assess potentially exposed individuals with no systematic starting point.
The IHR framework also provided the normative architecture for WHO's explicit advice against travel and trade restrictions, a position the organization maintained consistently throughout the response, formally stating that it "advises against the application of any travel or trade restrictions based on the current information available on this event." This guidance reflected both the scientific evidence about Andes virus transmission and the hard lessons of COVID-19, when disproportionate travel restrictions imposed by countries acting unilaterally caused enormous economic harm and public health disruption without meaningfully containing viral spread.
National Disease Agencies: South Africa, the Netherlands, and the Institut Pasteur de Dakar
The laboratory confirmation that transformed a cluster of unexplained deaths into a confirmed hantavirus outbreak came from South Africa, specifically from the National Institute for Communicable Diseases (NICD), which conducted PCR testing on samples from Case 2 and Case 3 and delivered the confirmation of hantavirus infection on 2 May 2026. This was the diagnostic breakthrough that reframed everything, retroactively reinterpreting Case 1's unexplained death at sea, triggering the IHR notification, and providing the laboratory foundation for every subsequent clinical and epidemiological decision. The NICD's continued role in sequencing, serology, and metagenomics was equally vital: the genetic characterization of the outbreak strain was essential not only for confirming the Andes identification but for the phylogenetic analysis that might eventually determine whether any human-to-human transmission had occurred.
South Africa's contribution extended beyond laboratory work. The country received and provided intensive care for Case 3, the adult male evacuated from Ascension Island, whose survival, at the time of reporting, represented one of the few unambiguously positive outcomes of the outbreak. The ICU care provided at a South African facility, operating under infection control conditions appropriate for a confirmed hantavirus patient, demonstrated the kind of clinical capacity that makes a meaningful difference in a disease where the case fatality rate can reach 50 percent and where survival is almost entirely dependent on the quality and speed of supportive care.
The Netherlands, as the flag state of the MV Hondius and the home country of the ship's operating company Oceanwide Expeditions, carried its own distinct responsibilities in the response. Dutch authorities engaged through their National IHR Focal Point from the earliest stages, coordinating with WHO and partner nations on the management of the vessel and its passengers. Dutch doctors were among those deployed aboard the ship during its transit to Tenerife, and patients evacuated from the vessel were transferred to hospitals in the Netherlands for treatment, underscoring the Dutch national health system's role not only as a regulatory authority but as a direct clinical provider in the response.
The engagement of the Institut Pasteur de Dakar in Senegal as an additional laboratory hub for testing additional samples from symptomatic passengers was a strategically important decision that reflected both the geographic realities of the outbreak and WHO's deliberate effort to distribute testing capacity across the regional laboratory network rather than concentrate it in a single facility. With the vessel operating in the Atlantic, Dakar represented a logistically accessible and scientifically capable alternative to European or South American laboratories, and its inclusion in the testing architecture strengthened the redundancy and speed of the diagnostic system.
The European Centre for Disease Prevention and Control (ECDC) provided a further layer of regional coordination, working alongside WHO and European national health authorities to integrate surveillance data, support risk assessment, and ensure that the European countries receiving evacuated patients or hosting passengers returning from the voyage had access to the most current technical guidance. A European disease specialist was among those who boarded the ship in Cabo Verde, physically embedding European public health expertise at the point of greatest operational need.
Contact Tracing Operations: The Global Search for Exposed Passengers
Among the most operationally demanding elements of the entire response was the contact tracing effort, a multinational exercise in locating, assessing, and monitoring individuals who might have been exposed to Andes hantavirus during the voyage of the MV Hondius, or during the index cases' pre-boarding travel through South America.
The challenge was geometrically complex. The vessel had carried passengers of 23 nationalities on a six-week voyage across the South Atlantic. Some had disembarked at intermediate ports, Saint Helena, Ascension Island, before the outbreak was formally recognized. Others remained aboard. Each passenger who had already returned home had traveled through international airports, sat on commercial flights, and potentially been in close contact with individuals, flight attendants, fellow passengers, taxi drivers, family members, who then required their own risk assessment. And all of this was unfolding against the backdrop of an incubation period that could extend to eight weeks, meaning that individuals who were exposed weeks ago might not yet show symptoms, while individuals who would never develop symptoms were generating unnecessary anxiety in healthcare systems not accustomed to managing hantavirus exposures.
WHO spokesperson Christian Lindmeier described the scope of the tracing effort in terms that captured both its ambition and its complexity: "It's following up on everybody. It's looking into seating lists of planes, of ships, maybe even more tracing somebody's steps, seeing where they would have been or might have been in close contact." The operational infrastructure for this effort, the airline seating records, the ship's manifest, the passenger embarkation and disembarkation logs at remote island ports, the flight connection data for individuals who transited through multiple hubs, had to be assembled rapidly across multiple jurisdictions, each with its own data protection frameworks and information-sharing protocols.
The flight attendant case served as the most publicly visible test of this tracing system, and provided the most reassuring result. The crew member who had come into close contact with Case 2, a visibly and severely ill passenger who died shortly afterward, was identified, tested, and confirmed negative for hantavirus. This outcome did more than any single epidemiological statement to demonstrate both the effectiveness of the contact tracing system and the limited transmissibility of the virus in non-household settings. It was, in WHO's telling, the most important negative result of the entire response.
WHO Representative Ann Lindstrand confirmed that national health authorities, coordinated by WHO, were systematically contacting passengers who had already disembarked to advise them to seek medical attention immediately if symptoms developed, and to ensure they understood what symptoms to watch for, over what time horizon, and with what degree of urgency. The 45-day active monitoring period recommended by WHO for all passengers and crew was not arbitrary; it reflected the outer bound of the documented Andes hantavirus incubation period, and it meant that the contact tracing and monitoring effort would continue for weeks after the vessel had docked and its passengers had dispersed.
The wife of one confirmed case, being treated in a Swiss hospital at the time of reporting, was self-isolating under monitoring, having had no symptoms despite the sustained intimacy of household contact. Her situation illustrated the dual function of contact tracing in this outbreak: it was simultaneously an epidemiological surveillance tool, generating data about transmission rates and secondary attack rates that would inform the scientific understanding of this event, and a public health protective measure, ensuring that individuals at elevated risk, however small that risk might be, were under observation and had immediate pathways to care if they needed it.
Governments: Solidarity, Sovereignty, and the Diplomacy of Quarantine
The governmental dimension of the MV Hondius response was, in some respects, the most politically consequential, and the most revealing about the fault lines that run through international outbreak management when abstract frameworks meet concrete political pressures.
| Country / Territory | Role in Response | Key Actions Taken | Outcome / Significance |
|---|---|---|---|
| United Kingdom | IHR notification state; administering authority for Saint Helena and Ascension Island | First country to notify WHO under IHR; initiated contact tracing for Case 2's flight to Johannesburg; administered territory at which Case 1's body was removed and Case 2 disembarked | Triggered the entire international response; IHR notification on 2 May 2026 was the legal and operational catalyst for global coordination |
| South Africa | Clinical care provider; primary diagnostic laboratory hub | Received Cases 2 and 3 via medical evacuation; NICD confirmed hantavirus by PCR; provided ICU care for Case 3; conducted sequencing and metagenomics | Laboratory confirmation transformed investigation from unexplained deaths to confirmed hantavirus cluster; Case 3's survival demonstrated value of advanced ICU capacity |
| Netherlands | Flag state of MV Hondius; national authority for Oceanwide Expeditions; receiving country for evacuated patients | Engaged National IHR Focal Point; deployed Dutch doctors aboard ship; received patients transferred to Dutch hospitals; coordinated with WHO and European partners | Flag state responsibilities created direct Dutch government accountability for vessel management and passenger welfare throughout the response |
| Argentina | Country of embarkation; most probable site of index case exposure; IHR information-sharing party | Shared passenger and crew lists with national IHR Focal Points according to each person's nationality; provided epidemiological context on ongoing Andes virus outbreak; sourced 2,500 diagnostic kits shipped by WHO to five countries | Manifest sharing was foundational to all subsequent national contact tracing operations; diagnostic kit provision strengthened multi-country testing capacity |
| Cabo Verde | Port state where vessel was moored at time of IHR notification | Declined to allow vessel to dock, citing public health concerns; cooperated with WHO experts boarding the ship; national health authorities coordinated with WHO on passenger assessment | Port refusal created diplomatic friction and logistical crisis; highlighted tension between sovereign port entry discretion and IHR norms discouraging disproportionate restrictions |
| Spain (Canary Islands) | Disembarkation host; diplomatic partner in WHO solidarity appeal | Agreed to allow MV Hondius to dock in Tenerife after WHO appeal to Prime Minister Sánchez; facilitated orderly disembarkation planning in coordination with WHO operational guidance | Spain's agreement resolved the immediate docking crisis; Dr. Tedros publicly credited PM Sánchez with an act of "solidarity" and "moral duty," establishing a diplomatic template for future port-of-refuge decisions |
| Switzerland | Receiving country for at least one confirmed case and close contacts | Hospitalized confirmed case; wife of patient self-isolating under monitoring with no symptoms reported | Demonstrated that European clinical systems were capable of managing confirmed Andes hantavirus cases under appropriate infection control conditions |
| Senegal | Regional laboratory partner | Institut Pasteur de Dakar engaged to receive and test additional samples from symptomatic passengers with WHO support | Expanded regional diagnostic redundancy; reduced dependence on South African and European laboratories for Atlantic-region samples |
The contrast between Cabo Verde's port refusal and Spain's acceptance was the defining diplomatic moment of the entire governmental response, and it crystallized, with unusual clarity, the tension that runs through every international outbreak involving a vessel at sea. Cabo Verde's decision was not irrational. A small island nation with limited healthcare infrastructure and a population acutely sensitive to the reputational and economic consequences of being associated with a disease outbreak had genuine domestic reasons to decline. The IHR framework, which advises against disproportionate restrictions but cannot compel sovereign port entry decisions, offered no mechanism to override that refusal.
Spain's willingness to step forward, driven by a direct WHO appeal to the highest level of government, resolved the immediate crisis and provided the narrative of international solidarity that Dr. Tedros needed to counterbalance the optics of a disease-stricken vessel turned away from port. "The risk to the people of the Canary Islands is actually low," Dr. Tedros said, framing Spain's decision not as a sacrifice but as an act consistent with the science, a contribution of political courage to a public health response that science alone could not complete.
The WHO Emergency Medical Team Secretariat worked in parallel with the EU Emergency Response Coordination Centre under a formal Working Arrangement to support the clinical management and medical evacuation of symptomatic passengers, a structural partnership between the UN system and European institutional infrastructure that, in this case, delivered tangible results in the form of coordinated evacuation logistics and medical support deployed to the vessel during its transit.
The Coordination Architecture: How the Pieces Fit Together
Mapping the full architecture of the multinational response reveals a system of considerable sophistication, and considerable fragility. The formal legal framework provided by the IHR created clear obligations and channels. The technical capacity of WHO and national disease agencies generated the diagnostic, epidemiological, and clinical intelligence that decision-makers needed. The political willingness of key governments, above all Spain, provided the physical infrastructure that made safe disembarkation possible. The operational presence of WHO experts aboard the ship ensured that the gap between Geneva's strategic direction and the reality aboard a vessel in the Atlantic was bridged by individuals with direct situational awareness.
But the system's vulnerabilities were equally on display. Cabo Verde's port refusal showed that the IHR's normative guidance can be overridden by sovereign discretion when domestic political pressures are sufficiently intense. The delay between Case 1's death on 11 April and the formal WHO notification on 2 May, nearly three weeks during which the ship continued its voyage without a confirmed hantavirus diagnosis, illustrated the limits of onboard medical capacity in remote expedition environments. The scale and complexity of the contact tracing operation, spanning 23 nationalities and multiple continents, strained the coordination mechanisms that the IHR provides but does not fully operationalize.
And the disinformation environment, the social media ecosystem in which every death, every port refusal, and every WHO press conference became raw material for pandemic-era catastrophism, placed demands on the communication function of every agency involved that were, in some respects, as challenging as the epidemiology itself. Dr. Tedros' observation that "viruses don't care about politics, and they don't care about borders" was accurate and eloquent. It was also, in the social media environment of 2026, insufficient on its own to close the gap between expert assessment and public fear, a gap that the multinational response team worked, with imperfect success, to narrow throughout the crisis.
What the MV Hondius response demonstrated, ultimately, was the indispensability of international cooperation in managing exactly this kind of event, and the persistent difficulty of achieving that cooperation reliably, consistently, and at the speed that a fast-moving outbreak demands. The system worked, in the sense that the outbreak was contained, patients received care, exposed individuals were traced and monitored, and the global public health risk remained low. But it worked despite its vulnerabilities as much as because of its strengths, and the gaps it revealed are ones that the next outbreak, arriving on a different vessel, carrying a different pathogen, docking at a different port, will exploit just as mercilessly as biology permits.
Cruise Travel and Infectious Disease Preparedness: Quarantine Protocols, Onboard Medical Screening, Isolation Measures, and International Coordination Lessons
The MV Hondius did not fail because the people aboard it were careless, or because the international response system was incompetent. It exposed something more uncomfortable than negligence: a structural mismatch between the infectious disease preparedness frameworks that govern maritime travel and the epidemiological realities of the modern cruise industry, particularly the expedition segment, which deliberately places passengers in the highest-risk ecological environments on Earth and then depends on institutional frameworks designed for a different era of travel to keep them safe.
Three people are dead. The global public health system mobilized across multiple continents. And the central question, one that no amount of diplomatic solidarity or WHO press briefings can answer on its own, is whether the frameworks governing onboard medical screening, quarantine protocols, isolation capacity, and international coordination are adequate for the disease risks that contemporary cruise travel, and expedition cruising in particular, actually generates. The evidence from the MV Hondius suggests they are not, and that the gap is not trivial.
Onboard Medical Capacity: The Structural Limits of Shipboard Healthcare
Every passenger ship operating under international maritime law is required to carry some form of medical capability. The precise requirements are set by flag state regulations, industry standards, and, for vessels operating internationally, the frameworks established under the International Maritime Organization's conventions and WHO's Handbook for Management of Public Health Events on Board Ships. In practice, what this means for most expedition cruise vessels is a ship's doctor or nurse, a medical bay with basic clinical equipment, and a pharmaceutical inventory calibrated to the kinds of illnesses that most commonly affect cruise passengers: gastrointestinal infections, respiratory viruses, cardiovascular events, traumatic injuries.
What it does not typically mean is the diagnostic infrastructure required to identify a rare zoonotic hemorrhagic virus in a patient presenting with nonspecific fever, headache, and diarrhea, which is precisely the clinical picture that Case 1 aboard the MV Hondius presented before he died. There is no point-of-care test for Andes hantavirus that can be operated aboard a ship. The PCR confirmation that identified the outbreak pathogen required specialized laboratory equipment available only at fixed facilities, in this case, the National Institute for Communicable Diseases in South Africa, following medical evacuation across international borders. The ship's medical team had no diagnostic pathway to hantavirus that could be activated in the field, in the middle of the South Atlantic, weeks from any laboratory capable of running the relevant assay.
This is not a criticism of the individuals providing care. It is a structural observation about the design of maritime medical systems, which are calibrated for the diseases that occur frequently enough to justify the investment in onboard diagnostic capability. Andes hantavirus is sufficiently rare that no plausible cost-benefit analysis would support installing PCR diagnostic equipment aboard every expedition cruise ship as a routine precaution. But that rarity calculation, which is correct in the aggregate, produces a specific and catastrophic failure mode in precisely the situations, like the MV Hondius, where the rare event actually occurs.
The practical consequence of this diagnostic gap was a three-week delay between the first death and the formal confirmation of hantavirus infection, three weeks during which the ship continued its voyage, passengers continued their normal social activities, and the possibility of a serious infectious disease cluster aboard was not formally recognized. Whether earlier diagnosis could have prevented subsequent deaths is impossible to determine with certainty. What is certain is that the absence of shipboard diagnostic capacity meant that the clinical and epidemiological picture remained invisible to the international public health system until the second patient collapsed on a commercial flight to Johannesburg.
Pre-Departure Screening: A Gap at the Point of Greatest Leverage
If there is a single point in the MV Hondius outbreak where a different intervention might have changed the trajectory of events, it is the embarkation process in Ushuaia on 1 April 2026. The index cases, the couple who would become Cases 1 and 2, had spent weeks traveling through Argentina, Chile, and Uruguay, visiting birdwatching sites in areas where the long-tailed pygmy rice rat, the primary reservoir of the Andes virus, is known to be present. Argentina was, at the time, experiencing an ongoing Andes virus outbreak with at least 20 documented deaths between July 2025 and January 2026 and a rising case fatality rate. That epidemiological context was not a secret; it was documented in Argentina's national health ministry data and circulated through PAHO's regional alert systems.
Yet no systematic pre-departure health screening was applied at embarkation designed to identify passengers with recent exposure to hantavirus-endemic environments. No structured questionnaire asked passengers whether they had visited rural areas, handled or come into contact with rodents, cleaned enclosed spaces in endemic regions, or experienced any fever or respiratory symptoms in the preceding weeks. No travel medicine advisory specific to Andes hantavirus risk was provided to passengers embarking on an expedition voyage departing from a region where the virus was actively circulating. And the incubation period of hantavirus, up to eight weeks, means that a passenger exposed days before boarding could be entirely asymptomatic at the point of embarkation, passing any fever screening without raising any flag.
This does not mean that comprehensive pre-departure screening would necessarily have prevented the outbreak. An asymptomatic individual in the incubation period cannot be identified by temperature checks or symptom questionnaires. But a structured hantavirus risk assessment at embarkation, focused on travel history and recent environmental exposures rather than current symptoms, could have flagged passengers with high-risk itineraries for enhanced monitoring during the voyage, ensuring that the ship's medical team was specifically alert to the possibility of hantavirus infection if those individuals developed fever or respiratory symptoms. In the case of Case 1, that enhanced clinical suspicion might have triggered earlier sample collection and emergency evacuation efforts before the disease reached its terminal cardiopulmonary phase.
WHO's formal outbreak guidance now specifically highlights the need for vigilance among travelers, crew, and personnel returning from areas where hantavirus is known to be present, with particular emphasis on conveyances engaged in ecotourism on journeys from and through those areas. The MV Hondius case will almost certainly accelerate industry and regulatory discussions about whether this vigilance requirement should be formalized into structured pre-embarkation screening protocols for expedition voyages departing from hantavirus-endemic regions, a step that falls well within operational feasibility even if it cannot provide complete epidemiological protection.
Isolation Infrastructure: The Arithmetic of Quarantine at Sea
When the outbreak aboard the MV Hondius was formally recognized, the primary isolation instruction issued to passengers was straightforward: remain in your cabins, maintain physical distancing, practice respiratory etiquette, and wear a medical mask if you develop respiratory symptoms. This instruction reflects both the genuine transmission biology of Andes hantavirus, which requires close, prolonged contact rather than airborne aerosol spread, and the practical reality of what isolation can look like aboard a vessel at sea.
The problem is that cabin isolation on a cruise ship, while meaningful, is not equivalent to clinical isolation in a hospital setting. Ventilation systems on ships typically recirculate air through shared ducts, though modern expedition vessels increasingly use individual cabin ventilation units. Shared bathrooms, common corridors, dining facilities, and galley services create contact pathways that cannot be entirely eliminated through voluntary cabin confinement, particularly on a small expedition vessel where the ship's crew must continue operating the ship regardless of passenger isolation instructions. The infection prevention and control environment aboard even a well-managed cruise ship is categorically different from a negative-pressure isolation room in an infectious disease ward.
For hantavirus specifically, a pathogen whose transmission requires prolonged close contact rather than casual proximity, this limitation may be less consequential than it would be for a more readily transmissible respiratory virus. The MV Hondius experience appeared to support this conclusion: cabin-sharing contacts of confirmed cases in some instances did not develop infection, and the outbreak did not amplify explosively through the vessel's remaining population despite the weeks during which the virus was present and the isolation measures were not yet in place. But this favorable outcome reflects the specific biology of Andes virus, not the adequacy of shipboard isolation infrastructure, and a different pathogen, with different transmission dynamics, would have exposed the same structural limitations in a far more damaging way.
The broader question for the industry is whether expedition cruise vessels operating in remote environments, weeks from any port, far beyond the reach of rapid medical reinforcement, should be required to maintain a dedicated isolation facility designed to clinical infection control standards: negative pressure capability, separate ventilation, anteroom for donning and doffing personal protective equipment, and medical monitoring capacity appropriate for a patient who might deteriorate rapidly and require resuscitation. WHO's Guide to Ship Sanitation and associated maritime health frameworks provide guidance on these questions, but the standards they establish reflect a baseline for conventional commercial vessels rather than the specific risk profile of expedition ships operating in zoonotic disease-endemic environments with limited evacuation options.
Medical Evacuation Logistics: The Tyranny of Geography
Among the operational challenges that the MV Hondius outbreak made viscerally apparent, perhaps none is more structurally intractable than the geography of medical evacuation from an expedition vessel following a remote itinerary. The ship's route, Antarctica, South Georgia, Nightingale Island, Tristan da Cunha, Saint Helena, Ascension Island, was specifically designed to take passengers to the least-accessible places on Earth. That is its commercial value proposition. It is also, in a medical emergency, an extreme operational liability.
Tristan da Cunha, one of the ship's planned stops, is the most remote permanently inhabited island in the world: 2,400 kilometers from Saint Helena, with no airstrip and a population of roughly 250 people whose medical facility consists of a small clinic. Nightingale Island is uninhabited. South Georgia has a research station but no hospital. In any of these locations, a passenger developing acute respiratory failure from hantavirus cardiopulmonary syndrome, a condition that can progress from nonspecific malaise to irreversible shock within hours, would have access to whatever the ship's medical bay could provide, and whatever emergency services could be organized across hundreds or thousands of nautical miles of open ocean.
Case 3's medical evacuation from Ascension Island to South Africa, a distance of approximately 3,400 kilometers, required a level of logistical coordination, aircraft availability, and South African ICU capacity that came together successfully in this instance. The WHO Emergency Medical Team Secretariat and the EU Emergency Response Coordination Centre engaged formally under their Working Arrangement to support clinical management and medical evacuation logistics. The patient survived, his condition improving in intensive care. But the margin between that outcome and the outcome that befell Case 1, who died at sea, undiagnosed, before any evacuation could be organized, may have been measured in hours and in the accident of geographic position at the moment of deterioration.
The MV Hondius case raises a question that the expedition cruise industry has not yet fully confronted: should vessels operating extreme remote itineraries, particularly those departing from or visiting zoonotic disease-endemic regions, be required to have pre-established, operationally tested medical evacuation protocols specifying, for each segment of the voyage, the nearest facility capable of providing ICU-level care for specific disease categories, the fastest available evacuation route to that facility, and the conditions under which evacuation should be initiated? The answer to that question, from a public health preparedness standpoint, appears clearly to be yes. The commercial and regulatory mechanisms for requiring it do not yet exist at the level of specificity the MV Hondius case suggests is necessary.
Comparing Preparedness Frameworks: What Cruise Travel Requires vs. What It Currently Has
| Preparedness Domain | Current Standard / Requirement | Gap Revealed by MV Hondius | Recommended Enhancement |
|---|---|---|---|
| Pre-embarkation health screening | Symptom-based screening (fever, active illness) at boarding; voluntary health declarations in some jurisdictions | No structured assessment of travel history for zoonotic disease exposure; asymptomatic incubating cases pass screening undetected | Mandatory travel history questionnaire for passengers departing from or transiting through zoonotic disease-endemic regions; targeted risk stratification for high-exposure itineraries |
| Onboard diagnostic capacity | Basic clinical assessment; limited point-of-care testing (influenza, COVID, malaria in some cases); no onboard PCR for rare zoonotic pathogens | Three-week delay between first death and laboratory confirmation; hantavirus invisible to shipboard medical team throughout | Expanded point-of-care testing panels for expedition vessels operating in endemic regions; real-time telemedicine consultation with specialist infectious disease services; rapid sample transfer protocols for early-stage unexplained severe respiratory illness |
| Clinical isolation facilities | Sick bay with basic isolation capacity; cabin confinement for suspected infectious cases; no standardized negative-pressure rooms on expedition vessels | Cabin isolation adequate for Andes virus given limited transmissibility, but structurally insufficient for higher-risk pathogens; shared ventilation systems create theoretical transmission pathways | Dedicated isolation suite with negative-pressure capability and separate ventilation mandated for expedition vessels operating in high-risk disease environments; clinical isolation protocols aligned with hospital infection control standards |
| Medical evacuation planning | General maritime emergency protocols; flag state and port state responsibilities; no disease-specific evacuation pathway requirements | Evacuation from ultra-remote stops (Tristan da Cunha, Nightingale Island) relies entirely on ad hoc coordination; significant delays possible; Case 1 died before evacuation could occur | Mandatory pre-voyage medical evacuation planning for each itinerary segment, specifying nearest ICU-capable facility, fastest evacuation route, and disease-specific trigger conditions; pre-established agreements with receiving hospitals in potential evacuation destinations |
| Crew and passenger health education | General hygiene briefings; safety drills; limited disease-specific pre-departure advisories in most jurisdictions | Passengers visiting hantavirus-endemic South American sites received no structured advisory about rodent exposure risks, hantavirus symptoms, or monitoring requirements | Mandatory pre-departure disease risk briefing for voyages departing from or visiting zoonotic disease-endemic regions; written symptom monitoring guidance with clear escalation thresholds distributed to all passengers |
| Onboard infection prevention and control (IPC) protocols | General maritime hygiene standards; WHO Guide to Ship Sanitation provides baseline framework | IPC measures not escalated until outbreak formally recognized, weeks after first death; environmental disinfection delayed; no systematic surveillance for syndromic clustering of respiratory illness among passengers | Prospective syndromic surveillance system for unexplained fever and respiratory illness aboard expedition vessels; automatic IPC escalation triggered by first case of severe unexplained respiratory illness regardless of diagnostic confirmation |
| IHR notification speed | States Parties required to notify WHO of potential public health emergencies of international concern within 24 hours of assessment | Formal notification to WHO occurred 21 days after first patient death; delay driven by absence of diagnostic confirmation rather than procedural non-compliance | Expedition vessel operators required to notify flag state IHR Focal Point of any unexplained severe respiratory death within 24 hours regardless of diagnostic status; flag state responsible for preliminary IHR assessment and notification without awaiting laboratory confirmation |
| Post-disembarkation monitoring | General travel health advisories; no standardized mechanism for tracking and monitoring passengers dispersed across multiple countries after a potential onboard exposure event | Contact tracing of 23 nationalities dispersed across multiple continents before formal outbreak recognition required extraordinary multinational coordination effort; some passengers potentially unreachable through existing systems | Digital passenger tracking mechanism activated automatically upon IHR notification of shipboard disease cluster; mandatory 45-day self-monitoring requirement with structured reporting pathway for all passengers and crew; WHO-coordinated multinational contact tracing framework pre-established for vessel outbreak scenarios |
The IHR Notification Gap: When the Legal Framework Meets Diagnostic Reality
One of the most instructive systemic failures revealed by the MV Hondius timeline is the gap between the IHR's notification requirements and the diagnostic prerequisites that, in practice, determine when notification actually occurs. The IHR requires States Parties to notify WHO of potential public health emergencies of international concern within 24 hours of assessment, a timeline designed to enable the earliest possible international response. But in the MV Hondius case, the formal notification to WHO did not occur until 2 May 2026, three weeks after Case 1 died aboard the vessel.
This was not a procedural violation. It was an entirely predictable consequence of the fact that hantavirus cannot be diagnosed without laboratory confirmation, laboratory confirmation requires sample collection and transport to a fixed facility, and the ship was operating in some of the most remote waters on Earth with no realistic pathway to expedited laboratory testing. The United Kingdom, which ultimately triggered the IHR notification as the administering authority for Saint Helena and Ascension Island, acted appropriately within the framework, but the framework itself was not designed to handle the scenario in which a ship's passenger dies of an unidentified infection at sea, the body is removed at a remote British Overseas Territory, and the diagnostic confirmation that would trigger the IHR clock does not arrive for weeks.
The gap this reveals is not in the IHR's legal text but in the practical mechanisms that connect a shipboard clinical event to the notification system. WHO's own outbreak documentation is explicit that the first formal notification came from the UK's National IHR Focal Point only after laboratory confirmation of hantavirus infection, confirmation that was itself only possible after a second patient had been medically evacuated to South Africa and tested at the NICD. In the interval between Case 1's death and that laboratory confirmation, the international public health system had no formal visibility into what was happening aboard the MV Hondius.
A reformed approach would require expedition vessel operators to notify their flag state's IHR Focal Point, without waiting for diagnostic confirmation, upon any unexplained death from severe acute respiratory illness aboard the vessel, triggering a preliminary IHR risk assessment based on clinical presentation and epidemiological context rather than laboratory diagnosis. For a Dutch-flagged vessel departing from Argentina during an active Andes virus outbreak, an unexplained death from rapid-onset respiratory failure in the first week of voyage should, under any rational system design, have generated an immediate IHR preliminary notification and a WHO risk assessment, not because the diagnosis was confirmed, but because the epidemiological context made zoonotic disease a plausible differential diagnosis that warranted international attention.
Ecotourism, Zoonotic Risk, and the Regulatory Vacuum
The structural challenge that underlies the MV Hondius outbreak is not specific to the Andes hantavirus or to the MV Hondius. It reflects a broader and growing tension between the expanding commercial footprint of ecotourism and adventure travel in zoonotic disease-endemic environments and the regulatory frameworks that govern health and safety in those activities.
Expedition cruising is not a cottage industry. The sub-Antarctic islands, the remote Atlantic territories, and the wilderness coastlines of South America visited by vessels like the MV Hondius attract a growing global market of affluent, wildlife-focused travelers whose itineraries increasingly intersect with rodent populations, bat colonies, primate habitats, and other zoonotic disease reservoirs that public health systems have historically monitored in the context of rural agricultural communities, not international tourists arriving by expedition ship. The regulatory frameworks that govern occupational health in forestry and agricultural settings in hantavirus-endemic regions have no meaningful analog in the expedition cruise sector.
UCLA infectious disease researcher Vaithi Arumugaswami captured this gap precisely in his assessment of the MV Hondius case: the incident is "a warning that the viruses should be monitored and that more research is needed to develop vaccines and treatments for them," but it is equally a warning that the interface between ecotourism and zoonotic disease reservoirs requires regulatory attention that it has not yet received. The passengers aboard the MV Hondius were not negligent. They visited the kinds of places that expedition cruises are specifically designed and marketed to visit. The risk they encountered was a foreseeable consequence of the activity, not an aberration, and the absence of any systematic framework for assessing, communicating, and mitigating that risk before passengers departed from Ushuaia is a regulatory gap, not an accident.
The practical implications extend to pre-travel health advisories, tour operator duty of care obligations, flag state requirements for vessels operating in endemic regions, and the question of whether ecotourism operators have an obligation to provide disease-specific risk briefings to travelers visiting environments where exposure to specific zoonotic pathogens is a documented possibility. WHO's formal advice now explicitly addresses this: "Vigilance among travellers, crew, including those involved in implementing ship sanitation measures, or other personnel returning from areas where hantavirus is known to be present, as well as on conveyances engaged in eco-tourism on a journey from and through those areas, is essential." That vigilance cannot be operationalized without the regulatory and commercial frameworks that make it a requirement rather than an aspiration.
International Coordination Lessons: What the MV Hondius Response Revealed About System Strengths and Weaknesses
The multinational public health response to the MV Hondius outbreak was, by many measures, impressive. WHO activated three-level coordination within hours of notification. The NICD in South Africa delivered laboratory confirmation within days of receiving samples. Argentina shared passenger manifests across 23 national focal points. The Institut Pasteur de Dakar was engaged as a regional laboratory partner. Spain opened its ports when Cabo Verde closed theirs. A WHO expert, Dutch doctors, and a European disease specialist boarded the ship in Cabo Verde and provided continuity of medical assessment during transit to Tenerife. Two thousand five hundred diagnostic kits were shipped from Argentina to five countries within days of the formal outbreak declaration. The contact tracing operation identified and assessed a flight attendant who had handled a critically ill patient and delivered a reassuring negative result within the critical early days of the response.
These are genuine achievements. They reflect decades of investment in IHR implementation, laboratory network development, WHO operational capacity, and the kind of multi-country trust relationships that make rapid information sharing possible in a crisis. The world was not flying blind, and that matters enormously in an outbreak where the difference between a contained cluster and a global epidemic is measured in hours of diagnostic and coordination speed.
But the weaknesses were equally visible, and they are weaknesses that the next outbreak, on the next vessel, carrying the next pathogen, will encounter unchanged unless specific remedial action is taken. The three-week diagnostic gap between first death and formal notification exposed the inadequacy of shipboard medical screening for rare zoonotic pathogens in expedition settings. Cabo Verde's port refusal demonstrated that IHR normative guidance cannot substitute for political will and that the international system has no effective mechanism for ensuring port access for disease-affected vessels when sovereign states decline. The complexity of tracing 23 nationalities dispersed across multiple continents before outbreak recognition illustrated that the IHR's notification and information-sharing mechanisms, while functional, were not designed for the speed and geographic dispersion that modern international travel creates. And the absence of any pre-existing mechanism for proactively notifying passengers who had already disembarked, before the formal WHO notification, meant that individuals with the highest potential exposure were the last to be systematically reached.
Each of these weaknesses has a potential remedy. Strengthened pre-embarkation screening requirements for voyages departing from endemic regions. Mandatory early IHR notification for unexplained severe respiratory deaths at sea, without awaiting diagnostic confirmation. Pre-established port-of-refuge agreements for disease-affected vessels, negotiated in advance through bilateral and multilateral diplomatic channels rather than assembled in crisis mode. Digital passenger tracking mechanisms activated automatically upon IHR notification, enabling immediate multinational contact tracing from a pre-existing technological platform rather than an ad hoc coordination effort. Expanded laboratory network arrangements enabling rapid sample analysis from remote maritime locations without dependence on patient evacuation as a prerequisite for diagnosis.
None of these remedies is simple, and none is cost-free. They require investment, regulatory reform, commercial cooperation, and the kind of sustained political attention that outbreak preparedness struggles to attract in the intervals between crises. The MV Hondius outbreak is, for the moment, a crisis with a low global risk assessment and a contained case count. Its political salience will fade. The question is whether the systemic lessons it has generated will be acted upon before the next expedition vessel, carrying the next pathogen, tests frameworks that remain, for now, essentially unchanged from the ones that allowed three people to die before the world formally learned the ship had a problem.
What Responsible Expedition Cruise Preparedness Should Look Like: A Framework
Drawing together the lessons of the MV Hondius case, the diagnostic gap, the evacuation logistics, the IHR notification delay, the pre-embarkation screening absence, the port refusal diplomacy, it is possible to sketch the architecture of a genuinely fit-for-purpose infectious disease preparedness framework for expedition cruise operations in zoonotic disease-endemic environments. It is not a framework that currently exists in any complete form. It is one that the MV Hondius has made it impossible to defer designing any longer.
At the pre-departure stage, the framework would require a voyage-specific disease risk assessment conducted by the operating company in consultation with the relevant national health authority and WHO regional office, identifying the specific zoonotic pathogens for which the itinerary creates meaningful exposure risk. For a voyage departing from Ushuaia during an active Andes virus outbreak, this assessment would generate a mandatory passenger health briefing covering hantavirus transmission routes, symptom recognition, the critical importance of disclosing recent rural travel history to the ship's medical team, and the 45-day monitoring requirement upon disembarkation. WHO's existing hantavirus outbreak toolbox provides the technical foundation for such briefings and should be incorporated into operator pre-departure protocols.
Aboard the vessel, the framework would establish a prospective syndromic surveillance system, a simple, structured daily reporting mechanism through which the ship's medical team tracks the incidence of fever, respiratory symptoms, and gastrointestinal illness among passengers and crew, with automatic escalation triggered by any clustering of unexplained severe respiratory illness. It would require dedicated isolation facilities meeting defined clinical infection control standards, with pre-positioned personal protective equipment appropriate for the zoonotic pathogens relevant to the itinerary. And it would establish a standing telemedicine arrangement with an infectious disease specialist at a named institution, enabling real-time clinical consultation for any passenger presenting with a syndrome that raises diagnostic uncertainty.
At the international coordination level, the framework would establish pre-agreed notification pathways requiring the vessel operator to notify the flag state's IHR Focal Point within 24 hours of any unexplained severe respiratory death aboard, and requiring the flag state to conduct a preliminary IHR risk assessment within a further 24 hours, generating a WHO notification if the epidemiological context warrants it, without awaiting laboratory confirmation. It would establish pre-negotiated port-of-refuge arrangements for disease-affected vessels operating in remote itineraries, agreed diplomatically in advance and activated automatically upon IHR notification, eliminating the improvised diplomatic scramble that the MV Hondius case required. And it would require the operating company to maintain a real-time digital manifest updated at each embarkation and disembarkation point, shareable with national IHR Focal Points within hours of a formal notification, enabling immediate multinational contact tracing from a complete and current data source.
These are not revolutionary proposals. They are extensions of principles that already exist in WHO guidance, maritime health frameworks, and IHR practice, applied with the specificity and operational rigor that the expedition cruise sector's unique risk profile demands. The MV Hondius has provided, at terrible cost to those aboard, the clearest possible demonstration of what happens when those principles are present in general guidance but absent in operational reality. Whether that demonstration is sufficient to drive the regulatory and commercial reform required is a question that governments, international bodies, and the expedition cruise industry itself will need to answer, before the next voyage departs from the next endemic port, carrying the next group of travelers who have no reason to know that the frameworks meant to protect them are not equal to the risks they are about to encounter.
What Travelers and the Public Should Know: Current Risk Assessment, Prevention Guidance, and Key Updates to Monitor
For the vast majority of people on Earth, the outbreak aboard the MV Hondius represents no direct personal threat. WHO has been unequivocal: the risk to the global population is "absolutely low," the virus does not spread like COVID-19, and the public health tools available to contain Andes hantavirus are well understood and demonstrably effective. But for specific categories of people, those who were aboard the MV Hondius, those who traveled through hantavirus-endemic areas of South America in recent weeks, those who came into close contact with affected passengers, and those planning future expedition travel to endemic regions, the picture is more nuanced and the information more urgent.
What follows is a clear, evidence-based account of the current risk assessment, the prevention measures that matter, and the developments that anyone following this outbreak should be tracking in the days and weeks ahead.
The Current WHO Risk Assessment: What "Low Global Risk" Actually Means
When WHO says the global public health risk from the MV Hondius hantavirus outbreak is low, that assessment rests on a specific set of biological and epidemiological facts, not on optimism, and not on a desire to avoid public alarm. Understanding those facts is essential to interpreting the risk classification accurately.
First, hantavirus is not an airborne pathogen in the respiratory droplet sense. It does not spread through the kind of casual, brief, proximity-based contact that made SARS-CoV-2 capable of pandemic transmission. Human infection with the Andes strain requires either direct contact with infected rodent material, urine, feces, saliva, or close and prolonged contact with a symptomatic human patient. The evidence from the MV Hondius response has repeatedly illustrated this constraint in practice: a flight attendant who physically handled a critically ill, visibly deteriorating infected passenger tested negative; cabin-mates of confirmed cases in some instances remained uninfected; and the wife of a patient hospitalized in Switzerland had not developed symptoms despite the intimacy of sustained household contact. As WHO spokesperson Christian Lindmeier put it: "That should convince nearly everybody now that this is a dangerous virus, but only to the person who is really infected. And the risk to the general population remains absolutely low."
Second, the outbreak is contained within a defined, traceable population. The MV Hondius carried 147 people of 23 nationalities on a specific itinerary with documented port stops. The passenger and crew manifest has been shared with national IHR Focal Points. Contact tracing operations are active across multiple countries. The individuals at any meaningful potential risk are known, located, and under monitoring, they are not an anonymous community of millions.
Third, WHO's acting director for epidemic and pandemic management Maria Van Kerkhove stated directly: "This is not SARS-CoV-2. This is not the start of a COVID pandemic. Hantaviruses have been around for quite a while. We know this virus. It does not spread the same way that coronaviruses do." The tools to break transmission chains, case isolation, contact tracing, clinical monitoring, are well established, well practiced, and working.
What the low-risk assessment does not mean is that the virus is harmless. For those who are infected, Andes hantavirus is a genuinely life-threatening pathogen with a case fatality rate that can reach 50 percent in the Americas and no approved specific antiviral treatment. The danger is real, it is simply not a danger that extends to the general public through casual exposure.
| Population Group | Current WHO Risk Level | Key Reason | Recommended Action |
|---|---|---|---|
| General global public with no connection to the outbreak | Negligible | No exposure pathway; virus requires close, prolonged contact or rodent exposure to transmit | Stay informed; no preventive action required beyond normal hygiene |
| Passengers who remained aboard MV Hondius until Tenerife | Low but active monitoring warranted | Potential shared environment exposure; incubation period still open for some | Active self-monitoring for 45 days from last potential exposure; seek immediate medical care if symptoms develop; disclose travel history |
| Passengers who disembarked at intermediate ports (Saint Helena, Ascension Island) before outbreak declaration | Low to moderate depending on individual exposure history | Aboard vessel during active case period; disembarked before formal monitoring began; incubation window may still be open | Contact national health authority immediately if not already done; self-monitor for 45 days from last date aboard vessel; seek care promptly if any symptoms appear |
| Close contacts of confirmed cases (household, healthcare workers providing care without full PPE) | Low but individually assessed | Transmission requires close and prolonged contact; documented negative results among contacts are reassuring but monitoring remains essential | Self-isolation; active symptom monitoring under health authority guidance; immediate testing if symptoms develop |
| Flight contacts of symptomatic passengers (fellow travelers, flight crew) | Very low | Flight attendant handling critically ill passenger tested negative; brief transit contact does not meet transmission threshold | Contact tracing notification if identified; routine symptom awareness; no preemptive isolation required in most cases per WHO guidance |
| Travelers recently returned from hantavirus-endemic South American regions (Argentina, Chile) | Low; dependent on activities | Endemic circulation ongoing in Argentina; exposure risk linked to specific rural, wildlife, or rodent-habitat activities, not general tourism | Monitor for symptoms for up to 45 days after return; disclose travel history to healthcare provider if seeking care for fever or respiratory symptoms; avoid rodent contact in endemic areas |
| Travelers planning future expedition travel to endemic regions | Low for standard tourism; elevated for rural, wildlife-immersive activities | Risk is activity-specific, not destination-specific; most routine tourism carries negligible exposure risk | Consult travel medicine specialist before departure; request pre-travel hantavirus risk briefing; understand symptoms and monitoring requirements; follow WHO prevention guidance for endemic areas |
Symptoms to Watch For: The Warning Signs That Demand Immediate Action
For anyone in a potentially exposed category, particularly former MV Hondius passengers or individuals who have recently traveled through rural or wildlife-rich areas of South America, knowing what symptoms to watch for, and understanding how little time there may be to act, is the single most important piece of practical information this outbreak has generated.
Andes hantavirus infection progresses through two clinical phases that are separated by a deceptive interval of apparent normality. According to WHO's clinical description, the initial prodromal phase, lasting approximately three to five days, presents with:
- Fever, typically high-grade and abrupt in onset
- Severe headache
- Muscle pain (myalgia), often described as intense and generalized
- Dizziness and chills
- Gastrointestinal symptoms, nausea, vomiting, diarrhea, abdominal pain
- Fatigue, often profound and disproportionate to apparent illness severity
These symptoms are nonspecific and easily misidentified as influenza, gastroenteritis, or a generic febrile illness. There are no respiratory symptoms at this stage, which is precisely what makes the prodromal phase so dangerous. A patient presenting with fever, muscle pain, and diarrhea has no obvious signal, absent a specific travel history, that they may be on the cusp of catastrophic respiratory failure.
The cardiopulmonary phase arrives with abrupt and devastating speed, typically within hours of the prodromal period ending. Its hallmarks are:
- Sudden onset of shortness of breath, rapidly progressive
- Cough
- Acute respiratory distress, lungs filling with fluid as vascular permeability collapses
- Hypotension and shock
- Rapid deterioration potentially requiring mechanical ventilation within hours
Without immediate access to intensive care, the cardiopulmonary phase is frequently fatal. This is the phase that killed Case 1 aboard the MV Hondius before he could be evacuated. It is the phase that killed Case 2 during a commercial flight. It is the phase from which Case 3 is recovering, having reached an ICU in South Africa in time to receive the ventilatory and hemodynamic support his survival required.
The critical clinical implication is this: do not wait for respiratory symptoms before seeking medical attention. Anyone in an at-risk category who develops fever, severe muscle pain, headache, and gastrointestinal symptoms after potential exposure should seek medical care immediately, disclose their travel history explicitly, and specifically raise the possibility of hantavirus with the treating clinician. Waiting until breathing becomes difficult may be waiting too long.
The incubation period, the time between exposure and first symptoms, ranges from one week to eight weeks, with most cases presenting within two to four weeks. WHO has specifically warned that the Andes hantavirus incubation window means additional cases may still emerge among those exposed during the voyage. For MV Hondius passengers, the monitoring clock is 45 days from the date of last potential exposure.
Prevention: What Actually Works Against Andes Hantavirus
Because there is no approved vaccine and no licensed antiviral treatment for Andes hantavirus cardiopulmonary syndrome, prevention, both of initial rodent-to-human transmission and of the limited human-to-human spread the virus is capable of, is the only reliable form of protection. The good news is that the preventive measures for both transmission routes are practical, well-understood, and highly effective when applied consistently.
Preventing Rodent-to-Human Transmission
The primary route of human hantavirus infection is inhalation of aerosolized rodent excreta, dust contaminated with the urine, feces, or saliva of an infected rodent. WHO's specific guidance for travelers in endemic regions covers the following essential practices:
- Avoid contact with rodents and their nesting materials. Do not handle live or dead rodents, disturb rodent nests, or enter enclosed spaces with evidence of rodent infestation without appropriate protective equipment.
- Use wet-cleaning methods, never dry sweeping. Sweeping contaminated surfaces aerosolizes rodent excreta and dramatically increases inhalation risk. Wet mopping with disinfectant solution, or using a spray bottle to dampen surfaces before cleaning, suppresses aerosolization. The US CDC provides detailed guidance on safe rodent cleanup procedures that is fully applicable to travelers in endemic environments.
- Ensure adequate ventilation in any enclosed spaces, cabins, outbuildings, field stations, before entering, particularly if the space has been closed for an extended period.
- Store food in rodent-proof containers to avoid attracting rodents and contaminating food supplies.
- Wear appropriate protective equipment, gloves, N95 or equivalent respirator, and protective eyewear, when working in environments with known rodent activity, cleaning areas with evidence of rodent infestation, or handling potentially contaminated materials.
- Avoid camping or sleeping in areas with visible rodent activity, burrows, droppings, nesting materials, particularly in South American wilderness environments where Oligoryzomys longicaudatus, the Andes virus reservoir, is present.
Crucially, WHO notes that most routine tourism activities carry little or no risk of exposure. Walking through a national park, visiting an urban area, or engaging with a wildlife guide in a structured ecotourism setting does not constitute meaningful hantavirus exposure risk. The danger is specific: it arises from close contact with rodent habitats, contaminated enclosed spaces, or the animals themselves, circumstances that are relevant to wilderness camping, agricultural work, and the kind of immersive birdwatching travel that the MV Hondius index cases engaged in, but not to the vast majority of tourism activities in South America.
Preventing Human-to-Human Transmission in Care Settings
For healthcare workers and household contacts of confirmed or suspected Andes hantavirus cases, the infection prevention and control requirements are more demanding. WHO's formal IPC guidance specifies:
- Standard precautions for all patient contacts: thorough hand hygiene, appropriate use of personal protective equipment, respiratory hygiene, and safe handling of blood and body fluids.
- Transmission-based precautions in addition to standard precautions for all suspected or confirmed cases, including gloves, gown, eye protection, and a well-fitted medical mask as a minimum.
- Airborne precautions, adding a fitted respirator (N95 or equivalent) and a negative-pressure room where available, for any aerosol-generating procedures such as intubation, bronchoscopy, or high-flow oxygen therapy.
- Prompt transfer to ICU when HPS is suspected, given the rapidity of potential cardiopulmonary deterioration and the life-saving importance of early advanced supportive care.
For household contacts of confirmed cases who are not themselves symptomatic, WHO's guidance based on the known transmission biology of Andes virus is more permissive than the post-COVID public intuition might suggest. Transmission requires close and prolonged contact, the kind sustained over days rather than hours. Household contacts should self-monitor actively, practice good hand hygiene, avoid sharing food and utensils with the symptomatic patient, and use a medical mask in close contact situations. But they do not, under current WHO guidance, require isolation equivalent to that applied to confirmed cases, provided they remain asymptomatic.
Diagnosis: How Hantavirus Infection Is Confirmed and Why Early Testing Matters
For anyone in an at-risk category who presents to a healthcare facility with fever, myalgia, and gastrointestinal symptoms after potential exposure, the diagnostic pathway is specific and time-sensitive. According to WHO's clinical guidance, hantavirus infection is confirmed by two primary laboratory methods:
- Serologic testing for IgM antibodies (indicating acute infection) or rising IgG antibody titres over sequential samples, using enzyme-linked immunoassay (ELISA). IgM antibodies are typically detectable at or shortly after symptom onset in most patients.
- Reverse transcriptase polymerase chain reaction (RT-PCR) to detect viral RNA, the method used to confirm hantavirus infection in Cases 2 and 3 aboard the MV Hondius. PCR is most sensitive during the prodromal phase, before significant antibody production has occurred.
The practical implication for patients is that disclosure of travel history to a treating clinician is not optional, it is diagnostically essential. A patient presenting with fever and myalgia who does not disclose recent travel through South American wilderness areas, or prior boarding of the MV Hondius, will almost certainly not prompt a clinician to order hantavirus testing as an early diagnostic priority. The differential diagnosis, influenza, dengue, leptospirosis, typhoid, is broad, and hantavirus testing requires specific awareness of exposure risk to be included in the initial workup. Tell your doctor where you have been, what you have done, and when symptoms began. That information may be the difference between a timely diagnosis and a preventable deterioration.
There is no approved specific antiviral treatment for hantavirus cardiopulmonary syndrome. Ribavirin, which has limited efficacy against the Old World hemorrhagic fever with renal syndrome syndrome, has not demonstrated effectiveness against HCPS and is not recommended. Treatment is entirely supportive, careful fluid management, hemodynamic monitoring, respiratory support, mechanical ventilation if required, and in severe cases extracorporeal membrane oxygenation (ECMO). This means that the quality and speed of access to an ICU-capable facility is the single most important determinant of survival outcomes. Early presentation, early diagnosis, and early transfer to intensive care capabilities are not optional enhancements, they are the treatment.
For Travelers: Pre-Travel Advice and What to Do Before Visiting Endemic Regions
The MV Hondius outbreak has direct relevance for anyone planning travel to hantavirus-endemic areas of South America, Argentina, Chile, Bolivia, Paraguay, Uruguay, and parts of Brazil, particularly those contemplating ecotourism, wildlife observation, wilderness camping, or any activity that involves time in rural environments, field stations, or natural habitats where rodent populations are present.
WHO's current surveillance data confirms that Argentina experienced at least 20 Andes virus deaths between July 2025 and January 2026, with a case fatality rate significantly above historical norms. As Nature reported, the fatality rate reached 34% between January 2025 and January 2026, well above the historical national average of 10–32%, suggesting that current conditions in Argentina represent an elevated rather than baseline risk environment for travelers with relevant exposure activities.
Before departing for endemic regions, travelers should:
- Consult a travel medicine specialist at least four to six weeks before departure. Request a specific briefing on hantavirus risk relevant to your planned activities and itinerary, not all travel medicine consultations include zoonotic disease risk assessment as standard unless it is explicitly requested.
- Understand what activities create meaningful exposure risk. Visiting Buenos Aires, hiking on well-maintained trails, or taking a structured urban or coastal tour does not constitute significant hantavirus exposure. Cleaning rural outbuildings, camping in areas with rodent activity, handling wildlife, or spending extended time in enclosed spaces with evidence of rodent infestation in endemic regions does.
- Know the symptoms and the monitoring requirements. If you engage in activities that constitute meaningful exposure risk, be prepared to self-monitor for up to 45 days after return and to seek medical attention promptly, not reactively, if fever, muscle pain, or gastrointestinal symptoms develop.
- Pack appropriate protective equipment if your activities require it: gloves, N95 respirator, and disinfectant supplies for cleaning enclosed spaces in endemic areas.
- Inform your healthcare provider upon return from endemic travel if you engaged in high-risk activities, so that any subsequent febrile illness is evaluated with appropriate clinical suspicion.
For those considering expedition cruise travel to the sub-Antarctic or South Atlantic on vessels departing from South American ports, the MV Hondius case provides a specific and urgent set of questions to raise with the operating company before booking:
- Does the operator provide a pre-departure disease risk briefing specific to the itinerary, including hantavirus risk for voyages departing from Argentina?
- What is the onboard medical capability for severe respiratory illness, and what are the evacuation pathways from each segment of the itinerary?
- Is there a structured syndromic surveillance system aboard the vessel?
- What are the operator's IHR notification protocols for unexplained severe illness at sea?
The absence of satisfactory answers to these questions is itself informative about the degree of preparedness a particular operator has invested in, and should factor into any traveler's booking decision in a post-MV Hondius expedition cruise market.
Key Developments to Monitor in the Coming Days and Weeks
The MV Hondius outbreak is not over. The ship has docked in Tenerife, disembarkation is underway, and the immediate crisis phase of the response has passed its most acute stage. But several critical developments remain outstanding, and anyone following this story, whether as a potentially exposed traveler, a healthcare professional, a public health practitioner, or a member of the informed public, should be tracking the following:
| Development to Monitor | Why It Matters | Expected Timeframe | What to Watch For |
|---|---|---|---|
| Sequencing and phylogenetic analysis results from NICD South Africa and Institut Pasteur de Dakar | Will determine whether cases share a single exposure source (rodent) or whether any human-to-human transmission chains occurred; fundamentally changes the epidemiological assessment of the outbreak | Days to weeks | WHO Disease Outbreak Notice updates; NICD South Africa press releases; scientific preprint servers |
| New case reports among disembarked passengers | The 45-day incubation window means cases may still emerge among passengers who disembarked before the outbreak was declared; any new laboratory-confirmed case in a former passenger would extend the contact tracing effort | Ongoing through June–July 2026 | WHO situation reports; national health agency announcements in countries of passenger nationality |
| Condition of Case 3 (patient in South African ICU) | The surviving critically ill patient represents the most severe documented case of the outbreak; his clinical trajectory will inform understanding of treatment approaches and long-term outcomes | Ongoing | South African NICD updates; WHO situation reports |
| Environmental investigation results: where and how were index cases exposed? | Identifying the precise exposure site, pre-boarding in South America, during shore excursions, or aboard the vessel, is essential for preventing recurrence and for understanding the geographic spread of active Andes virus circulation | Weeks to months | WHO Disease Outbreak Notice corrigenda; Argentine Ministry of Health reporting; scientific publications |
| Disembarkation and passenger dispersal outcomes in Tenerife | The orderly, safe disembarkation of passengers from 23 nationalities under WHO operational guidance is a critical test of the logistics framework developed during the response; any failures or complications would have immediate public health consequences | Days | WHO operational updates; Spanish health authority announcements; Canary Islands regional health service communications |
| Updated WHO risk assessment | WHO has stated it will continue to monitor the epidemiological situation and update its risk assessment as more information becomes available; any upward revision would trigger significantly expanded response measures | Ongoing; updated as evidence warrants | WHO Disease Outbreak News page for this event; WHO social media and press briefings |
| Argentine Andes virus outbreak trajectory | Argentina's ongoing outbreak, with an above-average case fatality rate, is the epidemiological background against which the MV Hondius index cases most probably acquired infection; changes in its scope or geographic distribution affect risk assessment for all future travel to the region | Ongoing; weekly PAHO updates | PAHO epidemiological alerts; Argentine Ministry of Health weekly bulletins |
| Regulatory and industry response to MV Hondius preparedness gaps | Whether flag state authorities, international maritime bodies, and the expedition cruise industry take concrete steps to address the pre-embarkation screening, onboard diagnostic, and IHR notification gaps the outbreak has revealed will determine the baseline preparedness level for the next equivalent event | Months to years | IMO committee proceedings; flag state regulatory announcements; expedition cruise industry association statements; WHO guidance updates |
What WHO Is Doing, and What It Is Not Recommending
To cut through the noise of social media speculation and ensure the public has an accurate picture of the institutional response, it is worth being precise about what WHO is and is not currently recommending in the context of the MV Hondius outbreak.
WHO is doing:
- Coordinating closely under the IHR with Cabo Verde, Spain, the Netherlands, South Africa, the United Kingdom, Argentina, and the European Centre for Disease Prevention and Control
- Maintaining an expert presence aboard and in coordination with the MV Hondius throughout transit to Tenerife
- Overseeing comprehensive medical assessment of all passengers and crew
- Developing operational guidance for safe disembarkation and onward passenger travel
- Supporting national health authorities in contacting disembarked passengers to advise on symptom monitoring
- Distributing 2,500 diagnostic kits to five countries to strengthen testing capacity
- Monitoring the epidemiological situation for any evidence of changing risk
- Actively countering disinformation on social media through clear, evidence-based public communication
WHO is explicitly not recommending:
- Any travel or trade restrictions based on current information
- Quarantine or entry screening for travelers from countries involved in the response
- Suspension of cruise or expedition travel to or from any region
- Any general public health measures targeting the broader population beyond those in directly exposed categories
As WHO's Disease Outbreak Notice states explicitly: "WHO advises against the application of any travel or trade restrictions based on the current information available on this event." This is not a passive or reluctant position, it is an affirmative recommendation grounded in the scientific evidence about Andes virus transmission, the effectiveness of targeted containment measures, and the hard lessons of COVID-era over-restriction that caused enormous harm without equivalent epidemiological benefit.
The Bottom Line: What the Science Says, Plainly Stated
Three people are dead, and that is a genuine tragedy. The Andes hantavirus is a genuinely dangerous pathogen, one that kills up to half of those it infects in the Americas, for which there is no approved vaccine and no specific antiviral treatment, and which is the only member of its viral family known to spread, under certain conditions, between people. None of those facts are in dispute, and none of them should be minimized.
But the totality of the scientific evidence assembled during the response to the MV Hondius outbreak points in a direction that is, for the general public, fundamentally reassuring: this is a virus that requires sustained, intimate contact to spread between people; that does not transmit efficiently even among household contacts and close companions of confirmed cases; that has been circulating in South America for decades without generating pandemic transmission chains; and that the world's public health systems, imperfect as they demonstrably are, have the tools and the knowledge to contain.
Dr. Tedros' closing words at the 7 May WHO press briefing were neither dismissive of the danger nor alarmist about the risk: "Viruses don't care about politics, and they don't care about borders. The best immunity we have is solidarity." For the travelers, healthcare workers, and government officials navigating the practical realities of this outbreak, and for the public trying to understand what it means, that framing captures both the genuine stakes and the proportionate response those stakes demand: serious, coordinated, evidence-driven, and grounded in the understanding that fear, however understandable, is not a substitute for science.
Monitor the WHO Disease Outbreak News page for this event for the latest risk assessments, case counts, and operational updates as the response continues. If you believe you may have been exposed, contact your national health authority without delay.
Comments
Leave a Comment
Your comment will appear after moderation.